Balder Jan W, de Vries Jeroen K, Mulder Douwe J, Kamphuisen Pieter W
1 Section of Molecular Genetics, Department of Pediatrics, University of Groningen, University Medical Center Groningen, the Netherlands.
2 Department of Vascular Medicine, University of Groningen, University Medical Center Groningen, the Netherlands.
Eur J Prev Cardiol. 2017 Jul;24(10):1064-1070. doi: 10.1177/2047487317698585. Epub 2017 Mar 14.
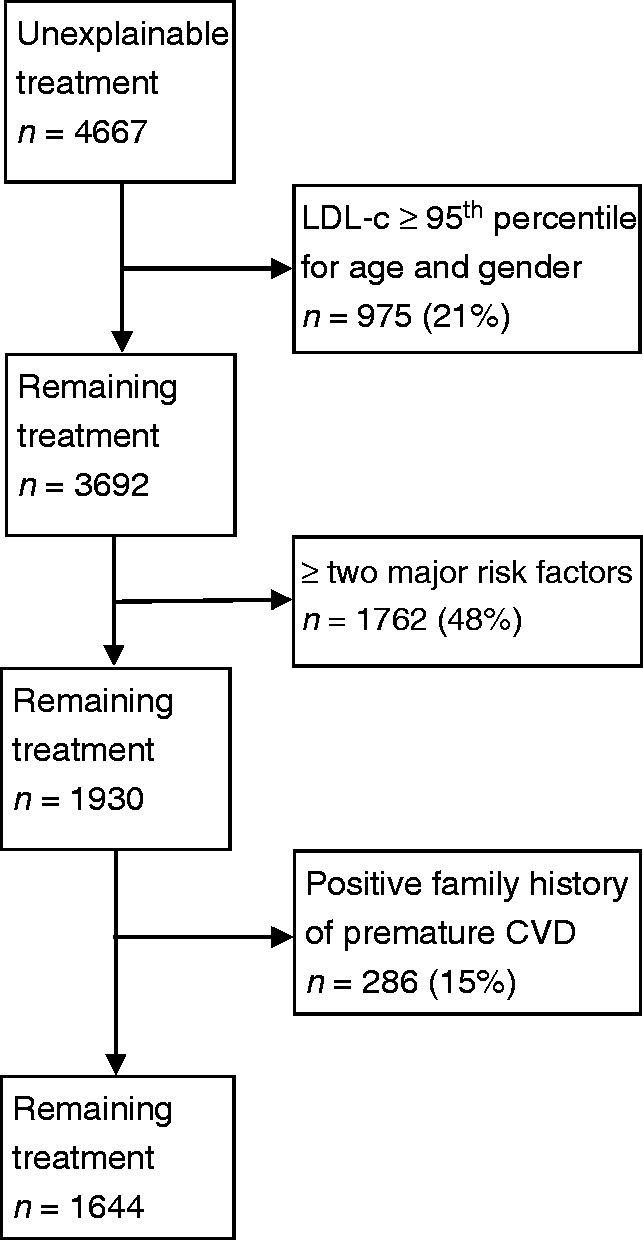
Background The challenge of the primary prevention of cardiovascular disease (CVD) is to identify patients who would benefit from treatment with statins. Statins are currently prescribed to many patients, even those at a low 10-year risk of CVD. These latter patients may not be eligible for statins according to current guidelines. Design This study investigated the prescription of guideline-consistent (according to guidelines) and guideline-inconsistent (not according to guidelines) lipid-lowering treatment in primary prevention in a large contemporary Dutch cohort study (Lifelines). Methods Lifelines is a large cohort study from the Netherlands. Participants were recruited between 2006 and 2013. They completed questionnaires and underwent a physical examination. Participants with previous CVD were excluded. Statins and ezetimibe were grouped as statin treatment. The Dutch guideline on cardiovascular management was used to assess eligibility for statins. Results Of 147,785 participants, 7092 (4.8%) reported statin treatment. In 4667 (66%) participants, statin treatment was inconsistent with the Dutch guideline. A total of 78% of these participants had a low 10-year predicted CVD risk. Multivariable logistic regression analysis showed that female sex and smoking were strongly associated with guideline-inconsistent treatment. Interestingly, 65% of the these participants had low-density lipoprotein cholesterol levels above the 95 percentile, adjusted for age and sex, two or more major risk factors of CVD or a positive family history of premature CVD. Therefore treatment might be reasonable. Conclusions There is a large inconsistency between guideline recommendations and the prescription of statins in clinical practice in the Netherlands. This is especially true for patients with low CVD risk. Many of these patients probably had risk-increasing circumstances justifying treatment.
背景 心血管疾病(CVD)一级预防面临的挑战是确定能从他汀类药物治疗中获益的患者。目前,许多患者都在服用他汀类药物,甚至包括那些10年心血管疾病风险较低的患者。根据现行指南,后一类患者可能不符合使用他汀类药物的条件。设计 在一项大型当代荷兰队列研究(生命线研究)中,本研究调查了一级预防中符合指南(根据指南)和不符合指南(不根据指南)的降脂治疗处方情况。方法 生命线研究是一项来自荷兰的大型队列研究。参与者于2006年至2013年招募。他们完成了问卷调查并接受了体格检查。既往有心血管疾病的参与者被排除。他汀类药物和依泽替米贝被归为他汀类治疗。采用荷兰心血管管理指南来评估使用他汀类药物的资格。结果 在147785名参与者中,7092名(4.8%)报告使用了他汀类药物治疗。在4667名(66%)参与者中,他汀类药物治疗不符合荷兰指南。这些参与者中共有78%的人10年预测心血管疾病风险较低。多变量逻辑回归分析表明,女性和吸烟与不符合指南的治疗密切相关。有趣的是,在这些参与者中,65%的人低密度脂蛋白胆固醇水平高于年龄和性别调整后的第95百分位数、存在两种或更多心血管疾病主要危险因素或有早发性心血管疾病家族史阳性。因此,治疗可能是合理的。结论 在荷兰的临床实践中,指南建议与他汀类药物处方之间存在很大不一致。对于心血管疾病风险较低的患者尤其如此。这些患者中的许多人可能有增加风险的情况,从而使治疗具有合理性。