O'Donnell Thomas F X, Deery Sarah E, Darling Jeremy D, Shean Katie E, Mittleman Murray A, Yee Gabrielle N, Dernbach Matthew R, Schermerhorn Marc L
Division of Vascular and Endovascular Surgery, Beth Israel Deaconess Medical Center, Boston, Mass.
Cardiovascular Epidemiology Research Unit, Department of Medicine, Beth Israel Deaconess Medical Center, Boston, Mass; Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, Mass.
J Vasc Surg. 2017 Aug;66(2):572-578. doi: 10.1016/j.jvs.2017.03.416. Epub 2017 May 12.
The 2013 American College of Cardiology/American Heart Association lipid management guidelines recommend high-intensity statins for all patients ≤75 years old with chronic limb-threatening ischemia (CLTI) and moderate-intensity statins for CLTI patients >75 years old without contraindications or on dialysis, but these recommendations are based primarily on coronary and stroke data. We aimed to validate these guidelines in patients with CLTI and to assess current adherence to these recommendations.
We identified all patients with CLTI who underwent first-time revascularization (endovascular or surgical) at Beth Israel Deaconess Medical Center from 2005 to 2014. Patients were classified as taking high-intensity, moderate-intensity, low-intensity, or no statin postoperatively. Outcomes included death and major adverse limb event (MALE). Propensity scores were calculated for the probability of receiving guideline-recommended intensity of statin therapy to account for nonrandom assignment of treatments. Cox regression models were constructed and adjusted for the propensity scores and further adjusted for strong potential confounders.
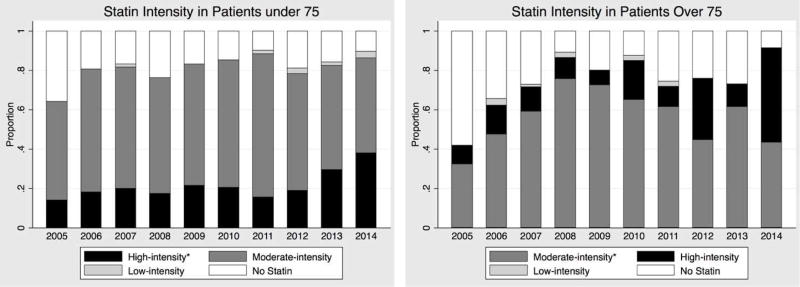
After excluding patients on hemodialysis (n = 252), we identified 1019 limbs from 931 patients with a median follow-up of 380 days. Patients discharged on the recommended statin intensity had higher rates of preoperative statin use, coronary artery disease, chronic kidney disease, stroke, atrial fibrillation, congestive heart failure, and coronary artery bypass grafting; they had lower smoking rates and were less likely to be ambulatory preoperatively. Overall, only 35% were taking the recommended statin dosage: 55% of those >75 years old and 20% of those ≤75 years old. In multivariable analysis including propensity scores where appropriate, discharge on any statin was associated with lower mortality (hazard ratio [HR], 0.71; 95% confidence interval [CI], 0.60-0.90; P < .01). Discharge on the recommended intensity of statin therapy was associated with lower mortality (HR, 0.73; 95% CI, 0.60-0.99; P < .05) and lower MALE rate (HR, 0.71; 95% CI, 0.51-0.97; P < .05). Patients >75 years old and ≤75 years old accrued similar benefit. In patients >75 years old, moderate-intensity statin therapy was associated with lower rates of death and MALE compared with high-intensity therapy but did not reach statistical significance.
Use of the recommended intensity of statin therapy in compliance with 2013 American College of Cardiology/American Heart Association lipid management guidelines is associated with significantly improved survival and lower MALE rate in patients undergoing revascularization for CLTI. Adherence to current guidelines is an appealing target for quality improvement.
2013年美国心脏病学会/美国心脏协会血脂管理指南建议,所有年龄≤75岁的慢性肢体威胁性缺血(CLTI)患者使用高强度他汀类药物,年龄>75岁且无禁忌证或未接受透析的CLTI患者使用中等强度他汀类药物,但这些建议主要基于冠心病和中风数据。我们旨在验证这些指南在CLTI患者中的有效性,并评估目前对这些建议的依从性。
我们确定了2005年至2014年在贝斯以色列女执事医疗中心首次接受血运重建(血管内或外科)的所有CLTI患者。患者术后被分类为服用高强度、中等强度、低强度或未服用他汀类药物。结局包括死亡和主要不良肢体事件(MALE)。计算倾向评分以确定接受指南推荐强度他汀治疗的概率,以考虑治疗的非随机分配。构建Cox回归模型,并根据倾向评分进行调整,进一步根据强潜在混杂因素进行调整。
排除接受血液透析的患者(n = 252)后,我们确定了931例患者的1019条肢体,中位随访时间为380天。出院时接受推荐他汀强度治疗的患者术前使用他汀类药物、冠心病、慢性肾病、中风、心房颤动、充血性心力衰竭和冠状动脉搭桥术的发生率较高;他们的吸烟率较低,术前步行的可能性较小。总体而言,只有35%的患者服用了推荐的他汀剂量:75岁以上患者中有55%,75岁及以下患者中有20%。在适当纳入倾向评分的多变量分析中,服用任何他汀类药物出院与较低的死亡率相关(风险比[HR],0.71;95%置信区间[CI],0.60 - 0.90;P <.01)。出院时接受推荐强度的他汀治疗与较低的死亡率相关(HR,0.73;95% CI,0.60 - 0.99;P <.05)和较低的MALE发生率相关(HR,0.71;95% CI,0.51 - 0.97;P <.05)。75岁以上和75岁及以下的患者获得了相似的益处。在75岁以上的患者中,中等强度他汀治疗与高强度治疗相比,死亡和MALE发生率较低,但未达到统计学意义。
按照2013年美国心脏病学会/美国心脏协会血脂管理指南使用推荐强度的他汀治疗与CLTI血运重建患者的生存率显著提高和MALE发生率降低相关。遵守现行指南是改善质量的一个有吸引力的目标。