Haland Trine F, Hasselberg Nina E, Almaas Vibeke Marie, Dejgaard Lars A, Saberniak Jørg, Leren Ida S, Berge Knut Erik, Haugaa Kristina H, Edvardsen Thor
Department of Cardiology, Institute for Surgical Research and Center for Cardiological Innovation, Oslo University Hospital, Rikshospitalet, Oslo, Norway.
University of Oslo, Norway.
Open Heart. 2017 May 16;4(1):e000571. doi: 10.1136/openhrt-2016-000571. eCollection 2017.
We explored cardiac volumes and the effects on systolic function in hypertrophic cardiomyopathy (HCM) patients with left ventricular hypertrophy (HCM LVH+) and genotype-positive patients without left ventricular hypertrophy (HCM LVH-).
We included 180 HCM LVH+, 100 HCM LVH- patients and 80 healthy individuals. End-Diastolic Volume Index (EDVI), End-Systolic Volume Index (ESVI) and ejection fraction (EF) were assessed by echocardiography. Left ventricular (LV) global longitudinal strain (GLS) was measured by speckle tracking echocardiography.
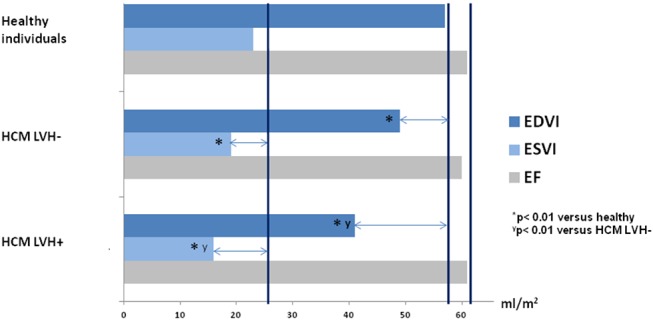
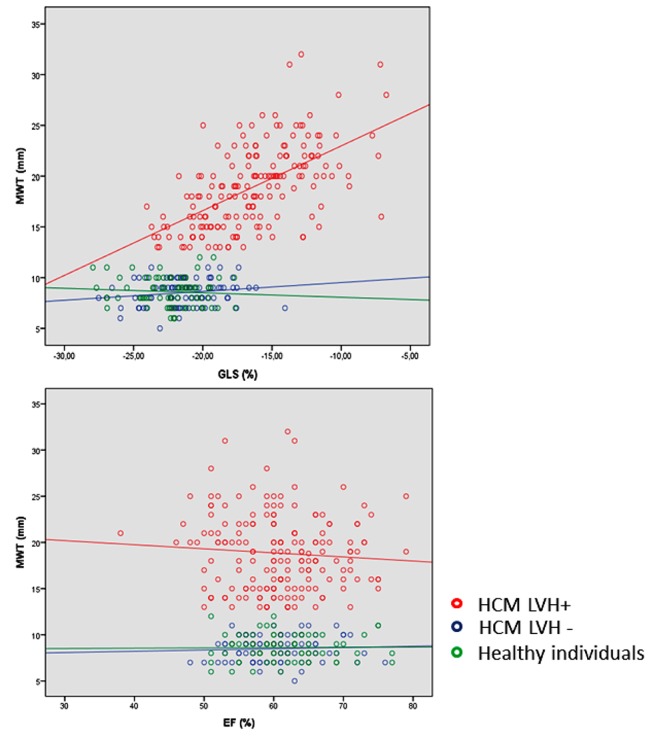
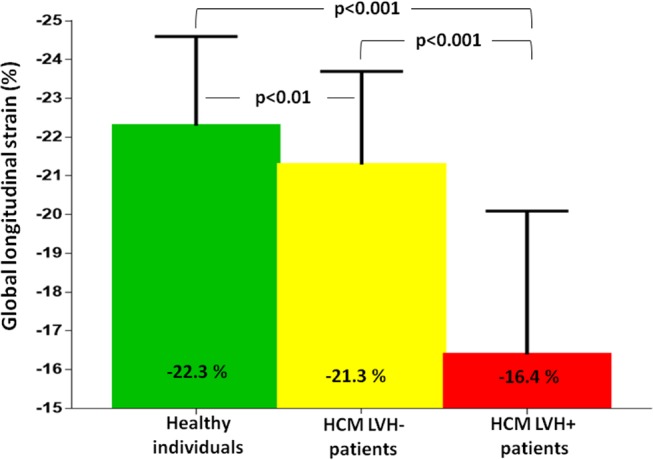
EDVI and ESVI were significantly smaller in HCM LVH+ compared with HCM LVH- patients (41±14 mL/m vs 49±13 mL/m and 16±7 mL/m vs 19±6 mL/m, respectively, both p<0.001) and in healthy individuals (41±14 mL/m vs 57±14 mL/m and 16±7 mL/m vs 23±9 mL/m, respectively, both p<0.001). HCM LVH- patients had significantly lower EDVI and ESVI compared with healthy individuals (49±13 mL/m vs 57±14 mL/m and 19±6 mL/m vs 23±9 mL/m, both p<0.001). EF was similar (61%±7% vs 60%±8% vs 61%±6%, p=0.43) in the HCM LVH+, HCM LVH- and healthy individuals, despite significantly worse GLS in the HCM LVH+ (-16.4%±3.7% vs -21.3%±2.4% vs -22.3%±3.7%, p<0.001). GLS was worse in the HCM LVH- compared with healthy individuals in pairwise comparison (p=0.001). Decrease in ESVI was closely related to EF in HCM LVH+ and HCM LVH- (R=0.45, p<0.001 and R=0.43, p<0.001) as expected, but there was no relationship with GLS (R=0.02, p=0.77 and R=0.11, p=0.31). Increased maximal wall thickness (MWT) correlated significantly with worse GLS (R=0.58, p<0.001), but not with EF (R=0.018, p=0.30) in the HCM LVH+ patients.
HCM LVH+ had smaller cardiac volumes that could explain the preserved EF, despite worse GLS that was closely related to MWT. HCM LVH- had reduced cardiac volumes and subtle changes in GLS compared with healthy individuals, indicating a continuum of both volumetric and systolic changes present before increased MWT.
我们探讨了肥厚型心肌病(HCM)合并左心室肥厚患者(HCM LVH+)和无左心室肥厚的基因型阳性患者(HCM LVH-)的心脏容积及其对收缩功能的影响。
我们纳入了180例HCM LVH+患者、100例HCM LVH-患者和80名健康个体。通过超声心动图评估舒张末期容积指数(EDVI)、收缩末期容积指数(ESVI)和射血分数(EF)。采用斑点追踪超声心动图测量左心室(LV)整体纵向应变(GLS)。
与HCM LVH-患者相比,HCM LVH+患者的EDVI和ESVI显著更小(分别为41±14 mL/m² 对49±13 mL/m² 和16±7 mL/m² 对19±6 mL/m²,均p<0.001),与健康个体相比也显著更小(分别为41±14 mL/m² 对57±14 mL/m² 和16±7 mL/m² 对23±9 mL/m²,均p<0.001)。与健康个体相比,HCM LVH-患者的EDVI和ESVI显著更低(49±13 mL/m² 对57±14 mL/m² 和19±6 mL/m² 对23±9 mL/m²,均p<0.001)。HCM LVH+、HCM LVH-患者和健康个体的EF相似(61%±7%对60%±8%对61%±6%,p=0.43),尽管HCM LVH+患者的GLS显著更差(-16.4%±3.7%对-21.3%±2.4%对-22.3%±3.7%,p<0.001)。在两两比较中,HCM LVH-患者的GLS与健康个体相比更差(p=0.001)。正如预期的那样,HCM LVH+和HCM LVH-患者中ESVI的降低与EF密切相关(R=0.45,p<0.001和R=0.43,p<0.001),但与GLS无关(R=0.02,p=0.77和R=0.11,p=0.31)。在HCM LVH+患者中,最大壁厚(MWT)增加与更差的GLS显著相关(R=0.58,p<0.001),但与EF无关(R=0.018,p=0.30)。
HCM LVH+患者的心脏容积更小,这可以解释其EF得以保留,尽管GLS更差且与MWT密切相关。与健康个体相比,HCM LVH-患者的心脏容积减小且GLS有细微变化,表明在MWT增加之前就存在容积和收缩功能变化的连续性。