De Both Anneleen, De Man Marc, Troisi Roberto, Van Vlierberghe Hans, Hoorens Anne, Geboes Karen
Department of Gastroenterology and Digestive Oncology, Ghent University Hospital, 9000 Ghent, Belgium.
Department of General, Hepato-Biliary and Liver Transplantation Surgery, Ghent University Hospital, 9000 Ghent, Belgium.
Oncol Lett. 2017 Jul;14(1):547-552. doi: 10.3892/ol.2017.6242. Epub 2017 May 24.
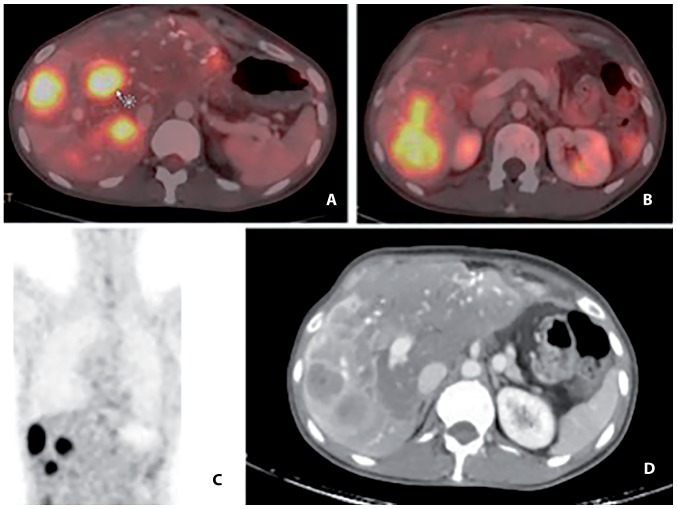
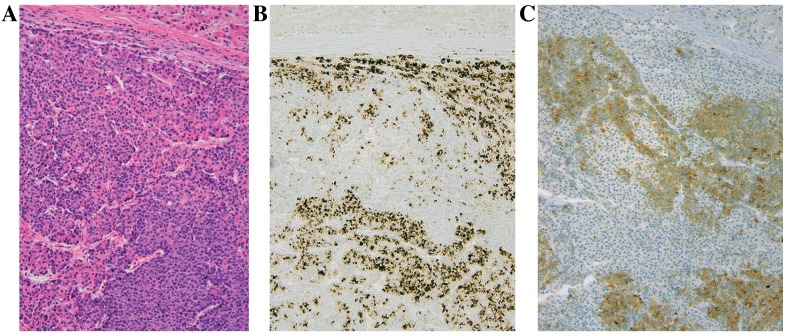
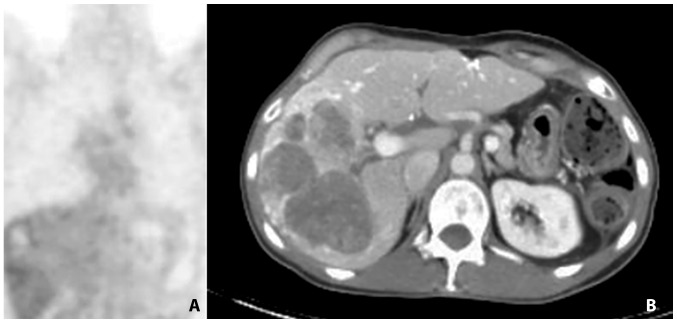
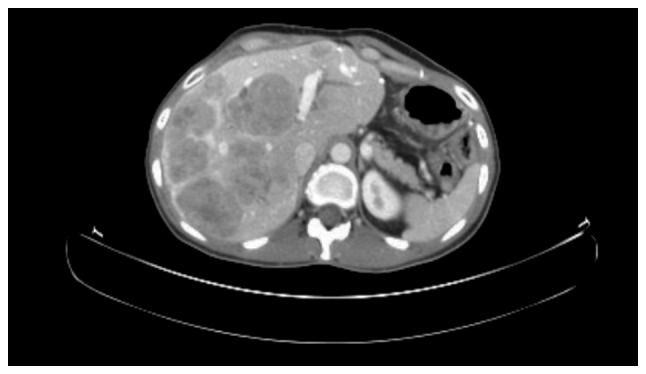
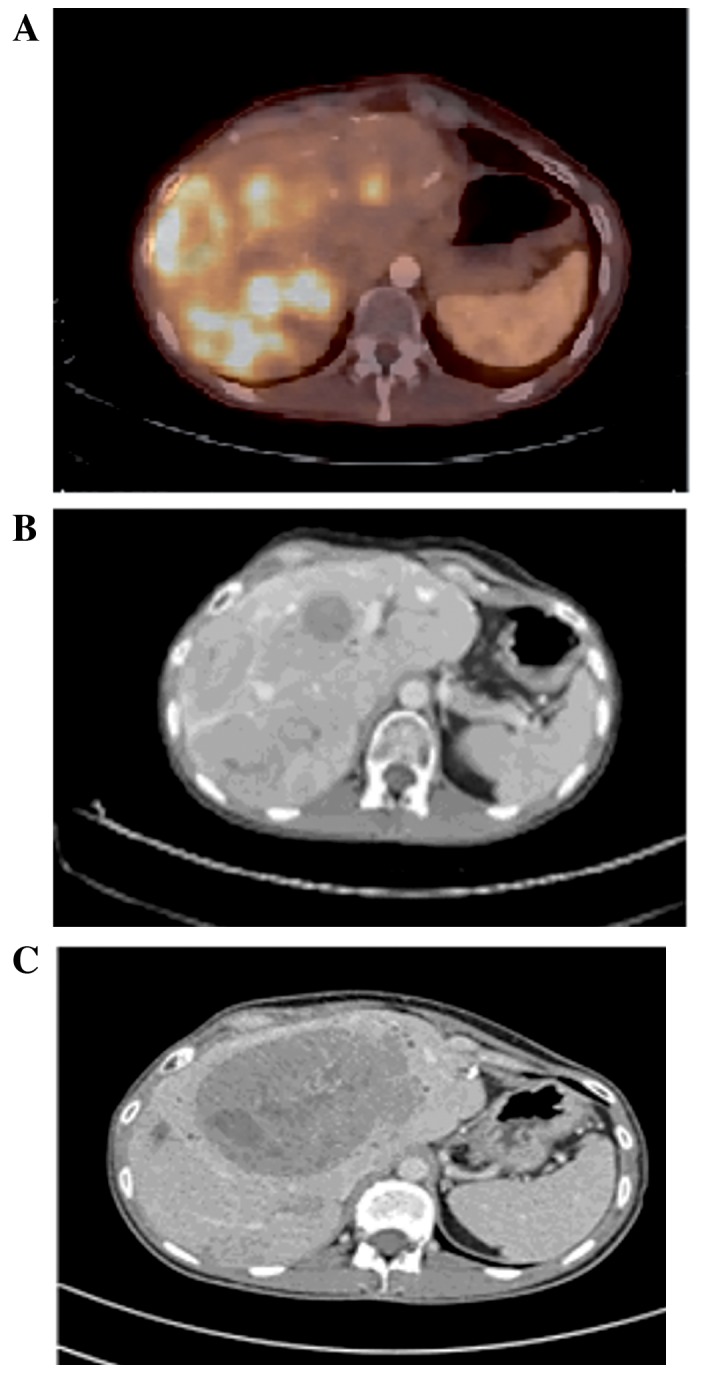
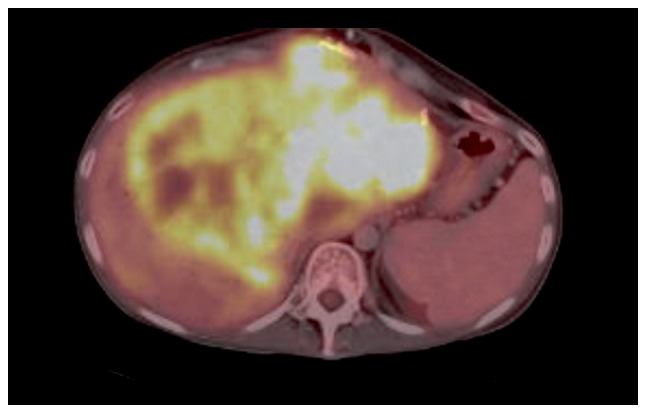
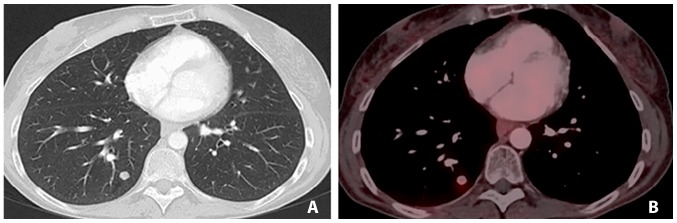
The case of a 35-year old female patient with a diagnosis of metastatic mixed acinar-endocrine carcinoma (MAEC) is investigated in the present study. The patient was believed to have a well-differentiated neuroendocrine tumor (NET) with a high Ki-67 index and uptake on Gallium-DOTATOC positron emission tomography-computed tomography for 9 years, and was treated accordingly. The patient had long lasting disease control by treatment with sunitinib, and a response was observed in numerous lesions with peptide receptor radionuclide therapy (PRRT). Following treatment for metastatic disease for >4 years, liver transplantation was performed, as an exception to normal recommendations, at the time of progression of a centrally located liver lesion inducing obstructive jaundice. Following transplantation, the diagnosis of a Grade 3 NET, as defined by the WHO 2010 classification, was challenged and changed to MAEC. MAEC is a rare type of tumor of the pancreas, exhibiting endocrine and acinar differentiation. It is difficult to diagnose, often being misidentified as acinar cell carcinoma or predominantly as neuroendocrine neoplasms. Immunohistochemical labelling provides the only evidence for the dual differentiation of neuroendocrine (synaptophysin and chromogranin) and acinar (lipase, trypsin and chymotrypsin) cell markers. Studies investigating MAECs with a clear histopathological diagnosis are scarce, in addition to evidence of disease behaviour and treatment options. It is generally agreed that surgery is the primary treatment in patients with resectable tumors. The responses to sunitinib and PRRT suggested that treatments considered or developed for NETs may be beneficial in MAEC cases.
本研究对一名35岁诊断为转移性混合性腺泡-内分泌癌(MAEC)的女性患者的病例进行了调查。该患者被认为患有高Ki-67指数的高分化神经内分泌肿瘤(NET),且在镓- DOTATOC正电子发射断层扫描-计算机断层扫描上有摄取,持续9年,并据此进行了治疗。患者通过舒尼替尼治疗实现了长期疾病控制,并且在肽受体放射性核素治疗(PRRT)中观察到许多病灶有反应。在转移性疾病治疗超过4年后,由于中央肝脏病变进展导致梗阻性黄疸,作为正常建议的例外情况,进行了肝移植。移植后,根据世界卫生组织(WHO)2010年分类定义的3级NET诊断受到质疑,并改为MAEC。MAEC是一种罕见的胰腺肿瘤类型,表现出内分泌和腺泡分化。其诊断困难,常被误诊为腺泡细胞癌或主要误诊为神经内分泌肿瘤。免疫组织化学标记是神经内分泌(突触素和嗜铬粒蛋白)和腺泡(脂肪酶、胰蛋白酶和糜蛋白酶)细胞标志物双重分化的唯一证据。除了疾病行为和治疗选择的证据外,对具有明确组织病理学诊断的MAEC进行研究的报道很少。一般认为,手术是可切除肿瘤患者的主要治疗方法。对舒尼替尼和PRRT的反应表明,针对NETs考虑或开发的治疗方法可能对MAEC病例有益。