Nasi D, Perano D, Ghadirpour R, Iaccarino C, Servadei F, Romano A
Neurosurgery-Neurotraumatology Unit of University Hospital of Parma, Parma and Department of Neurosurgery, Reggio Emilia, Italy.
Department of Otolaryngology Unit of Institute for Scientific and Care Research "ASMN" of Reggio Emilia, Reggio Emilia, Italy.
Surg Neurol Int. 2017 Jun 5;8:101. doi: 10.4103/sni.sni_450_16. eCollection 2017.
Neuroendocrine tumors (NET) originate from the diffuse neuroendocrine system. These can arise in almost every organ of the body, although they are most commonly found in the gastrointestinal tract and respiratory system. The skull base and sellar region are extremely rare sites for neuroendocrine carcinoma. Consequently, in this case, both diagnosis and definition of surgical goals, as well as further treatment strategies were challenging.
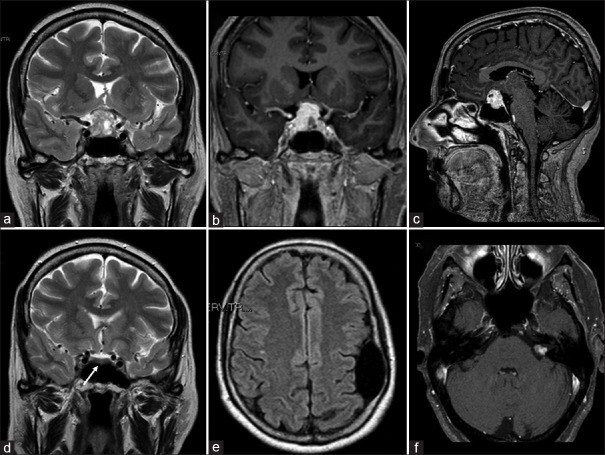
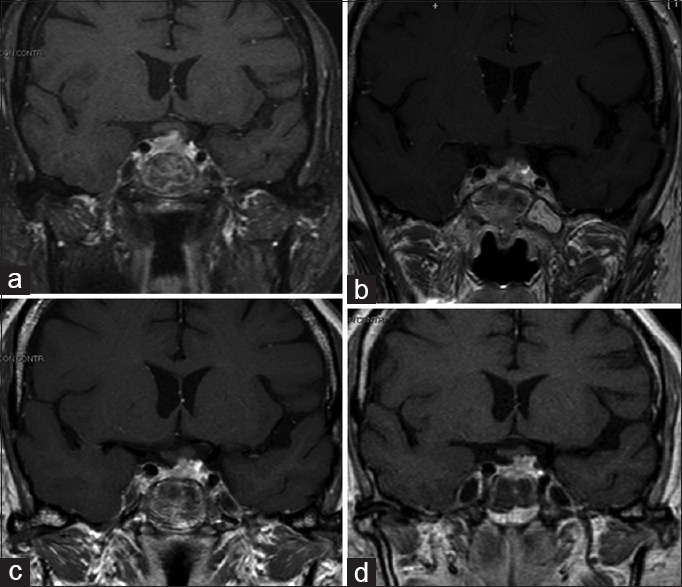
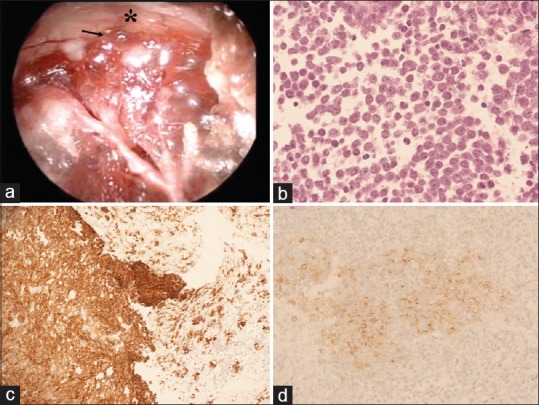
A 65-year-old woman was admitted to our Neurosurgery Department with a rapidly progressive visus reduction, drowsiness, polyuria, and polydipsia. Neuroimaging showed a sellar/suprasellar mass (diameter of 2 cm) with a heterogeneous signal compressing the optic chiasm and extending laterally toward the cavernous sinus. Differential diagnosis based on imaging included pituitary macroadenoma or metastasis. The patient underwent endoscopic endonasal transsphenoidal surgery. A total resection of the mass was impossible because of the infiltration of the optic chiasm and the intraoperative histological diagnosis of malignant epithelial neoplasm. Further histological evaluation revealed that the lesion was a NET with no other primary or metastatic sites detectable. Subsequently, the patient was successfully treated with fractioned stereotactic radiotherapy and polychemotherapy. Four years after the surgery, follow-up magnetic resonance imaging showed stability of the residual disease. Neurologic examination revealed a complete visual recovery.
Primary pituitary NET, though rare, should be included in the differential diagnosis of sellar lesions. A multimodality treatment approach is needed. Finally, the present case highlights, that in the case of a pituitary lesion infiltrating the optic chiasm, including NET, the endoscopic endonasal transsphenoidal subtotal resection followed by fractioned stereotactic radiotherapy and chemotherapy may represent an effective and safe choice of treatment.
神经内分泌肿瘤(NET)起源于弥散神经内分泌系统。尽管它们最常见于胃肠道和呼吸系统,但几乎可发生于身体的每个器官。颅底和鞍区是神经内分泌癌极为罕见的发病部位。因此,在本病例中,诊断、明确手术目标以及制定进一步的治疗策略均具有挑战性。
一名65岁女性因视力迅速下降、嗜睡、多尿和烦渴入住我院神经外科。神经影像学检查显示鞍区/鞍上有一肿块(直径2cm),信号不均匀,压迫视交叉并向外侧延伸至海绵窦。基于影像学的鉴别诊断包括垂体大腺瘤或转移瘤。患者接受了鼻内镜经蝶窦手术。由于视交叉受侵以及术中组织学诊断为恶性上皮性肿瘤,无法完全切除肿块。进一步的组织学评估显示该病变为神经内分泌肿瘤,未发现其他原发或转移部位。随后,患者成功接受了分次立体定向放疗和多药化疗。手术后四年,随访磁共振成像显示残留病灶稳定。神经系统检查显示视力完全恢复。
原发性垂体神经内分泌肿瘤虽罕见,但应纳入鞍区病变的鉴别诊断。需要采用多模式治疗方法。最后,本病例强调,对于浸润视交叉的垂体病变,包括神经内分泌肿瘤,鼻内镜经蝶窦次全切除后联合分次立体定向放疗和化疗可能是一种有效且安全的治疗选择。