Gupta Jhumka, Falb Kathryn L, Ponta Oriana, Xuan Ziming, Campos Paola Abril, Gomez Annabel Arellano, Valades Jimena, Cariño Gisele, Olavarrieta Claudia Diaz
Department of Global and Community Health, George Mason University, MS 5B7, 4400 University Drive, Fairfax, VA, 22030, USA.
International Rescue Committee, 122 East 42nd Street, New York, NY, 10168, USA.
BMC Med. 2017 Jul 12;15(1):128. doi: 10.1186/s12916-017-0880-y.
Rigorous evaluations of health sector interventions addressing intimate partner violence (IPV) in low- and middle-income countries are lacking. We aimed to assess whether an enhanced nurse-delivered intervention would reduce IPV and improve levels of safety planning behaviors, use of community resources, reproductive coercion, and mental quality of life.
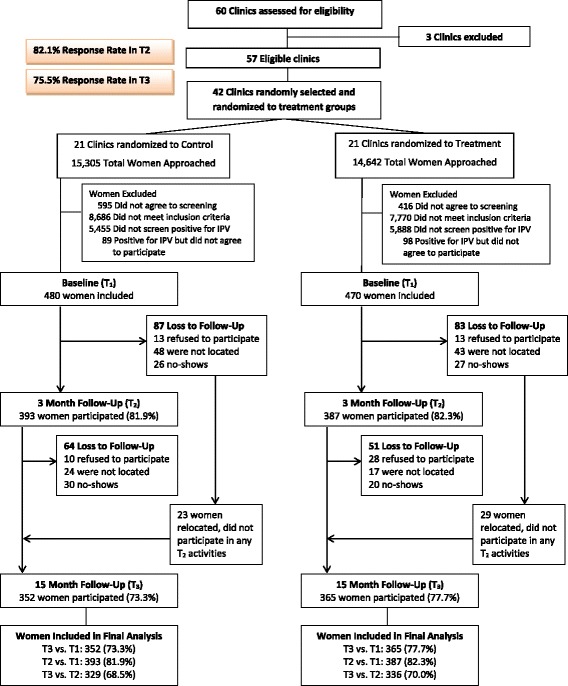
We randomized 42 public health clinics in Mexico City to treatment or control arms. In treatment clinics, women received the nurse-delivered session (IPV screening, supportive referrals, health/safety risk assessments) at baseline (T1), and a booster counselling session after 3 months (T2). In control clinics, women received screening and a referral card from nurses. Surveys were conducted at T1, T2, and T3 (15 months from baseline). Our main outcome was past-year physical and sexual IPV. Intent-to-treat analyses were conducted via three-level random intercepts models to evaluate the interaction term for treatment status by time.
Between April and October 2013, 950 women (480 in control clinics, 470 in treatment clinics) with recent IPV experiences enrolled in the study. While reductions in IPV were observed for both women enrolled in treatment (OR, 0.40; 95% CI, 0.28-0.55; P < 0.01) and control (OR, 0.51; 95% CI, 0.36-0.72; P < 0.01) clinics at T3 (July to December 2014), no significant treatment effects were observed (OR, 0.78; 95% CI, 0.49-1.24; P = 0.30). At T2 (July to December 2013), women in treatment clinics reported significant improvements, compared to women in control clinics, in mental quality of life (β, 1.45; 95% CI, 0.14-2.75; P = 0.03) and safety planning behaviors (β, 0.41; 95% CI, 0.02-0.79; P = 0.04).
While reductions in IPV levels were seen among women in both treatment and control clinics, the enhanced nurse intervention was no more effective in reducing IPV. The enhanced nursing intervention may offer short-term improvements in addressing safety planning and mental quality of life. Nurses can play a supportive role in assisting women with IPV experiences.
Clinicaltrials.gov ( NCT01661504 ). Registration Date: August 2, 2012.
在低收入和中等收入国家,针对亲密伴侣暴力(IPV)的卫生部门干预措施缺乏严格评估。我们旨在评估强化护士提供的干预措施是否能减少亲密伴侣暴力,并提高安全规划行为水平、社区资源利用、生殖胁迫及心理生活质量。
我们将墨西哥城的42家公共卫生诊所随机分为治疗组或对照组。在治疗诊所,女性在基线期(T1)接受护士提供的服务(IPV筛查、支持性转诊、健康/安全风险评估),并在3个月后(T2)接受强化咨询服务。在对照诊所,女性接受护士的筛查和转诊卡。在T1、T2和T3(基线期后15个月)进行调查。我们的主要结局是过去一年的身体和性方面的亲密伴侣暴力。通过三级随机截距模型进行意向性分析,以评估治疗状态随时间的交互项。
2013年4月至10月,950名有近期亲密伴侣暴力经历的女性(480名在对照诊所,470名在治疗诊所)参与了该研究。虽然在T3(2014年7月至12月)时,治疗组(OR,0.40;95%CI,0.28 - 0.55;P < 0.01)和对照组(OR,0.51;95%CI,0.36 - 0.72;P < 0.01)诊所的亲密伴侣暴力都有所减少,但未观察到显著的治疗效果(OR,0.78;95%CI,0.49 - 1.24;P = 0.30)。在T2(2013年7月至1