Kataoka Jun, Nitta Toshikatsu, Inoue Yoshihiro, Ota Masato, Tominaga Tomo, Fujii Kensuke, Kawasaki Hiroshi, Ishibashi Takashi
Department of Gastroenterological Center Surgery, Shunjukai Shiroyama Hospital, Osaka, Japan.
Department of General and Gastroenterological Surgery, Osaka Medical College Hospital, Osaka, Japan.
J Surg Case Rep. 2017 Jun 23;2017(6):rjx106. doi: 10.1093/jscr/rjx106. eCollection 2017 Jun.
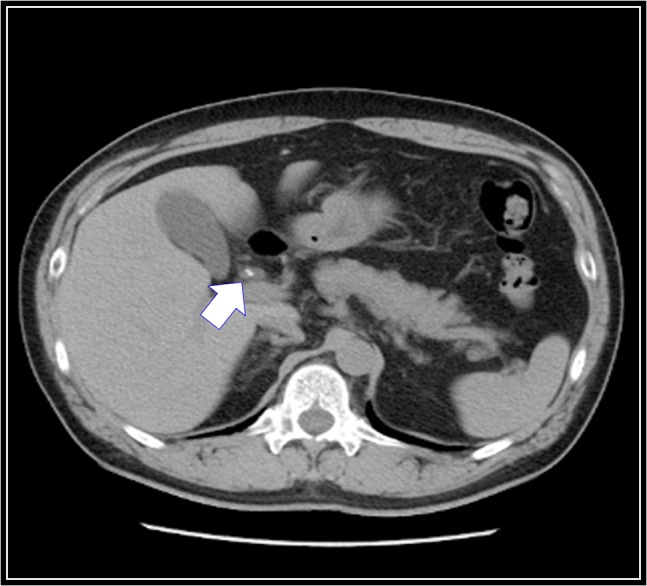
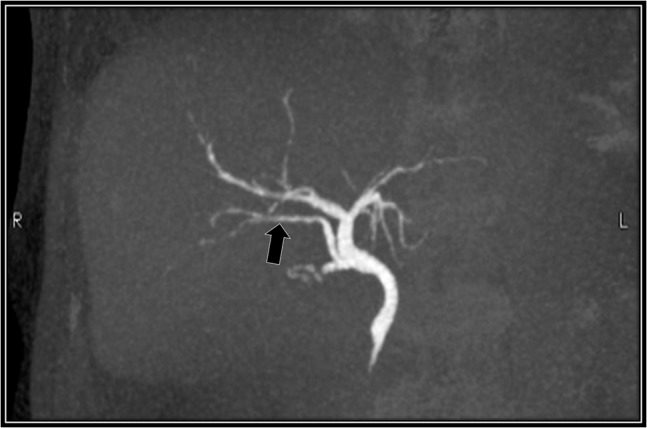
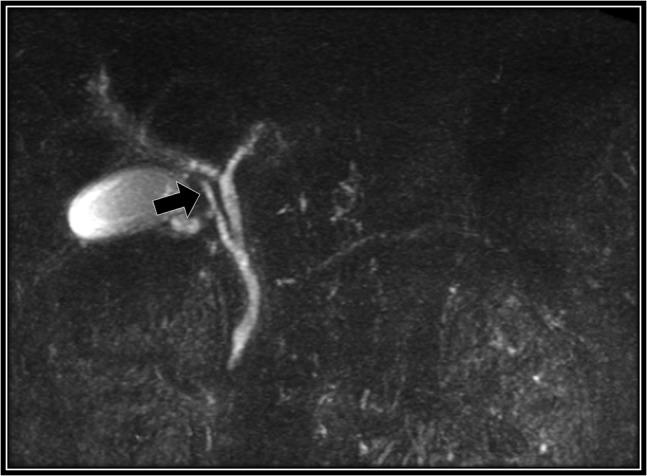
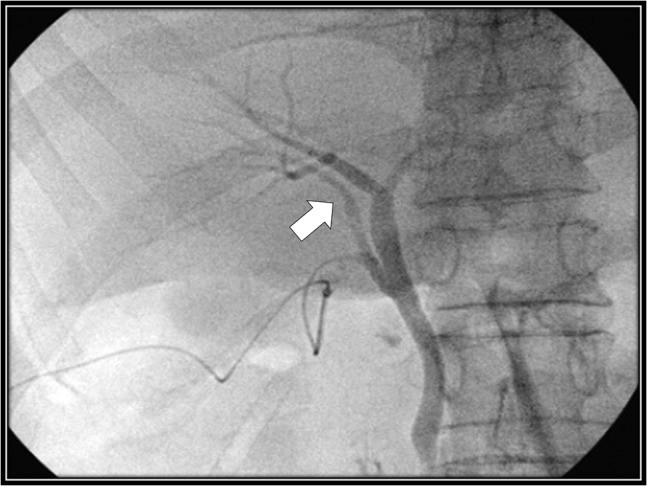
We describe a 48-year-old man with cholecystolithiasis whose preoperative magnetic resonance cholangiopancreatography (MRCP) scan showed that the right accessory hepatic duct branching from the cystic duct dominated an anterior segment of the right hepatic lobe. We observed the right accessory hepatic duct using intraoperative cholangiography, and we were able to perform laparoscopic cholecystectomy without injuring it. He had no complication after discharge, and a drip-infusion cholangiography-computed tomography (DIC-CT) scan demonstrated that the right accessory hepatic duct was intact, and it dominated an anterior segment of the right hepatic lobe. During laparoscopic cholecystectomy, a bile duct injury is the most challenging perioperative complication. We selected MRCP preoperatively; however, if it is necessary for us to observe an anomalous biliary tract more precisely, we recommend selecting DIC-CT endoscopic retrograde cholangiopancreatography. Additionally, we think a bile duct injury can be avoided with intraoperative cholangiography, even if there is an anomalous biliary tract.
我们描述了一名患有胆囊结石的48岁男性,其术前磁共振胰胆管造影(MRCP)扫描显示,从胆囊管分支的右副肝管支配右肝叶的前段。我们在术中胆管造影时观察到了右副肝管,并成功实施了腹腔镜胆囊切除术,未对其造成损伤。出院后他没有出现并发症,滴注式胆管造影计算机断层扫描(DIC-CT)显示右副肝管完好无损,且支配右肝叶的前段。在腹腔镜胆囊切除术中,胆管损伤是最具挑战性的围手术期并发症。我们术前选择了MRCP;然而,如果我们需要更精确地观察异常胆道,我们建议选择DIC-CT或内镜逆行胰胆管造影。此外,我们认为即使存在异常胆道,术中胆管造影也可以避免胆管损伤。