Bryson Christine, Boynton Greta, Stepczynski Anna, Garb Jane, Kleppel Reva, Irani Farzan, Natanasabapathy Siva, Stefan Mihaela S
a Department of Medicine, Division of Hospital Medicine , Baystate Medical Center , Springfield , MA , USA.
b Department of Medicine , Tufts University School of Medicine , Boston , MA , USA.
Hosp Pract (1995). 2017 Oct;45(4):135-142. doi: 10.1080/21548331.2017.1353884. Epub 2017 Jul 28.
To evaluate whether implementation of a geographic model of assigning hospitalists is feasible and sustainable in a large hospitalist program and assess its impact on provider satisfaction, perceived efficiency and patient outcomes.
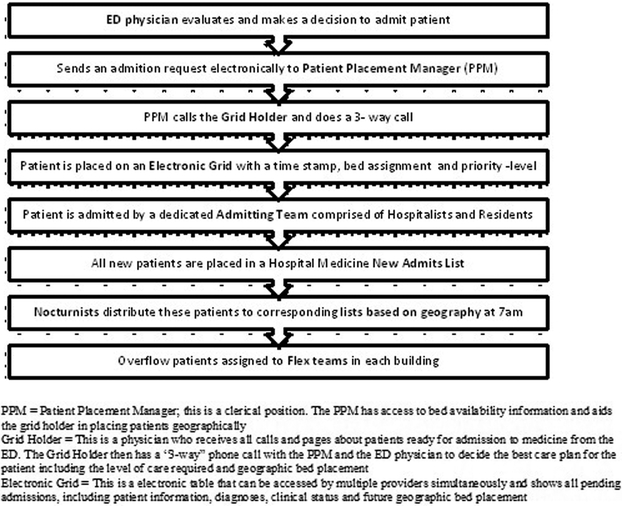
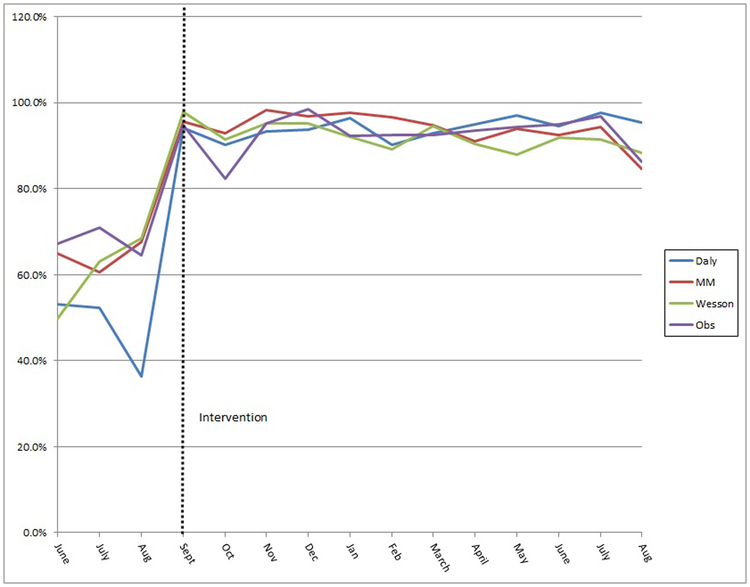
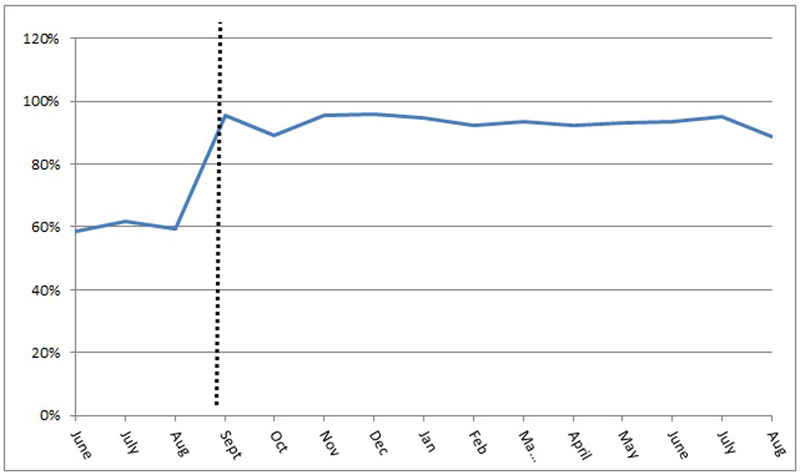
Pre (3 months) - post (12 months) intervention study conducted from June 2014 through September 2015 at a tertiary care medical center with a large hospitalist program caring for patients scattered in 4 buildings and 16 floors. Hospitalists were assigned to a particular nursing unit (geographic assignment) with a goal of having over 80% of their assigned patients located on their assigned unit. Satisfaction and perceived efficiency were assessed through a survey administered before and after the intervention.
Geographic assignment percentage increased from an average of 60% in the pre-intervention period to 93% post-intervention. The number of hospitalists covering a 32 bed unit decreased from 8-10 pre to 2-3 post-intervention. A majority of physicians (87%) thought that geography had a positive impact on the overall quality of care. Respondents reported that they felt that geography increased time spent with patient/caregivers to discuss plan of care (p < 0.001); improved communication with nurses (p = 0.0009); and increased sense of teamwork with nurses/case managers (p < 0.001). Mean length of stay (4.54 vs 4.62 days), 30-day readmission rates (16.0% vs 16.6%) and patient satisfaction (79.9 vs 77.3) did not change significantly between the pre- and post-implementation period. The discharge before noon rate improved slightly (47.5% - 54.1%).
Implementation of a unit-based model in a large hospitalist program is feasible and sustainable with appropriate planning and support. The geographical model of care increased provider satisfaction and perceived efficiency; it also facilitated the implementation of other key interventions such as interdisciplinary rounds.
评估在大型住院医师项目中实施基于地理位置分配住院医师的模式是否可行且可持续,并评估其对医疗服务提供者满意度、感知效率和患者结局的影响。
2014年6月至2015年9月在一家三级医疗中心进行了干预前后(前3个月 - 后12个月)的研究,该中心有一个大型住院医师项目,负责照顾分散在4栋楼和16层的患者。住院医师被分配到特定的护理单元(按地理位置分配),目标是使其80%以上的指定患者位于其指定单元。通过干预前后进行的一项调查评估满意度和感知效率。
按地理位置分配的比例从干预前的平均60%增加到干预后的93%。负责一个32张床位单元的住院医师数量从干预前的8 - 10人减少到干预后的2 - 3人。大多数医生(87%)认为地理位置对整体护理质量有积极影响。受访者表示,他们觉得地理位置增加了与患者/护理人员讨论护理计划的时间(p < 0.001);改善了与护士的沟通(p = 0.0009);并增强了与护士/病例管理人员的团队合作意识(p < 0.001)。实施前后的平均住院时间(4.54天对4.62天)、30天再入院率(16.0%对16.6%)和患者满意度(79.9对77.3)没有显著变化。中午前出院率略有提高(47.5% - 54.1%)。
在大型住院医师项目中实施基于单元的模式,通过适当的规划和支持是可行且可持续的。基于地理位置的护理模式提高了医疗服务提供者的满意度和感知效率;它还促进了其他关键干预措施的实施,如跨学科查房。