Department of Obstetrics and Gynecology, VU University Medical Center, Amsterdam, The Netherlands.
Department of Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands.
Ultrasound Obstet Gynecol. 2018 Mar;51(3):313-322. doi: 10.1002/uog.18809. Epub 2018 Feb 5.
Doppler ultrasonographic assessment of the cerebroplacental ratio (CPR) and middle cerebral artery (MCA) is widely used as an adjunct to umbilical artery (UA) Doppler to identify fetuses at risk of adverse perinatal outcome. However, reported estimates of its accuracy vary considerably. The aim of this study was to review systematically the prognostic accuracies of CPR and MCA Doppler in predicting adverse perinatal outcome, and to compare these with UA Doppler, in order to identify whether CPR and MCA Doppler evaluation are of added value to UA Doppler.
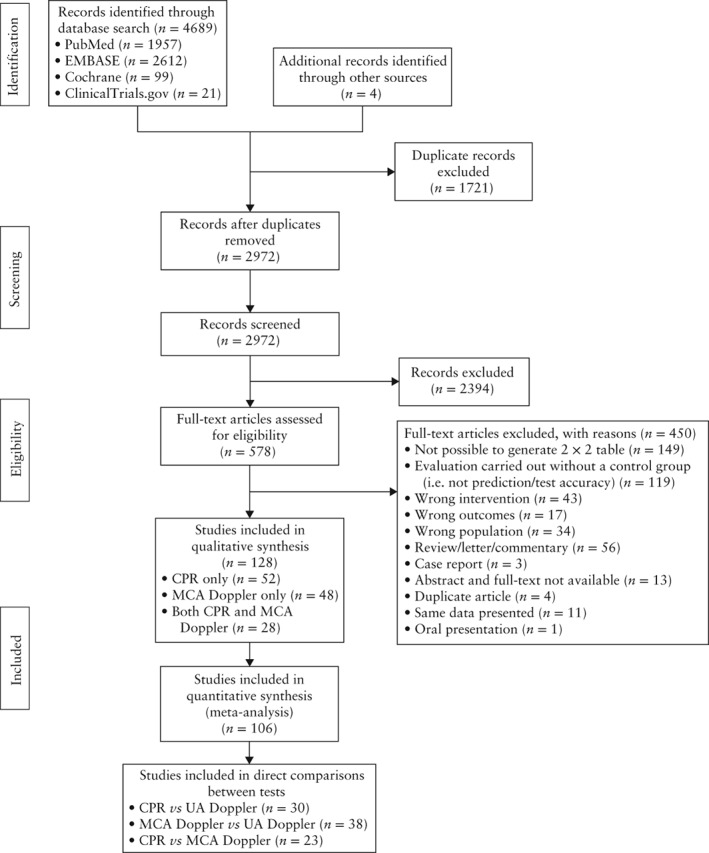
PubMed, EMBASE, the Cochrane Library and ClinicalTrials.gov were searched, from inception to June 2016, for studies on the prognostic accuracy of UA Doppler compared with CPR and/or MCA Doppler in the prediction of adverse perinatal outcome in women with a singleton pregnancy of any risk profile. Risk of bias and concerns about applicability were assessed using the QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies-2) tool. Meta-analysis was performed for multiple adverse perinatal outcomes. Using hierarchal summary receiver-operating characteristics meta-regression models, the prognostic accuracy of CPR vs MCA Doppler was compared indirectly, and CPR and MCA Doppler vs UA Doppler compared directly.
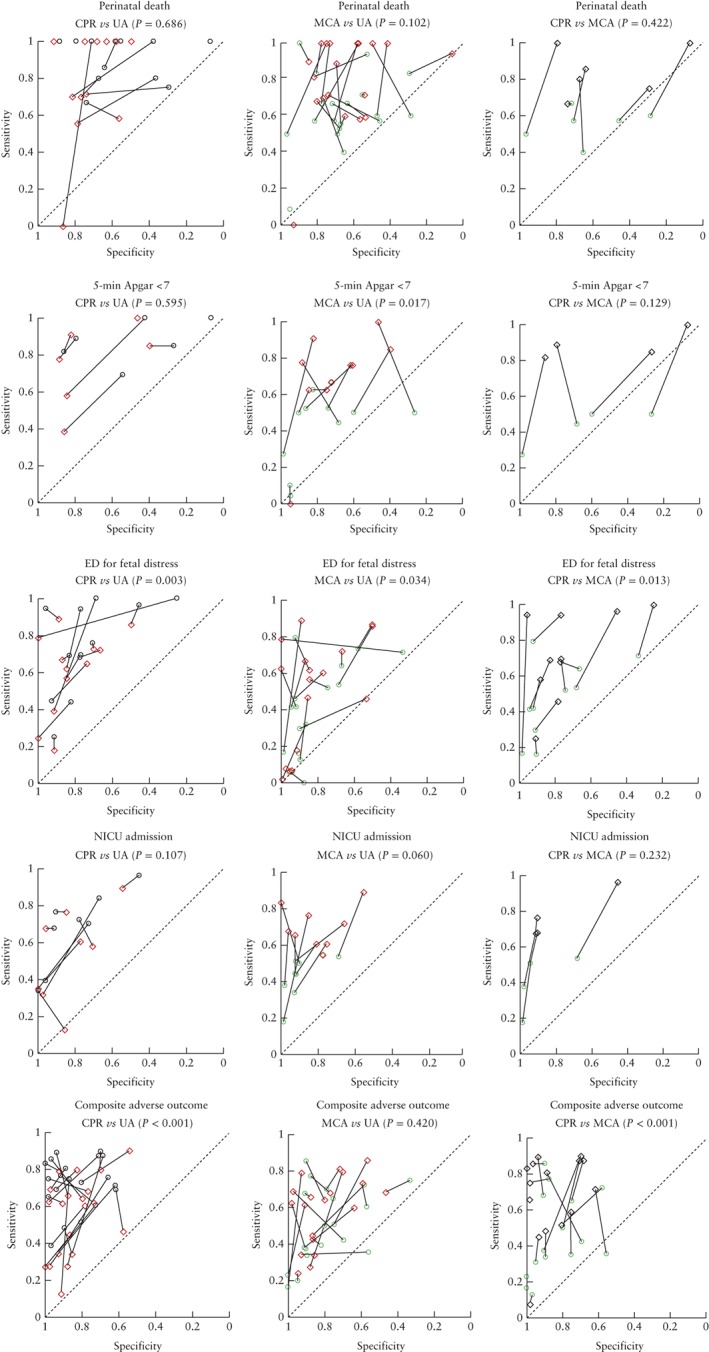
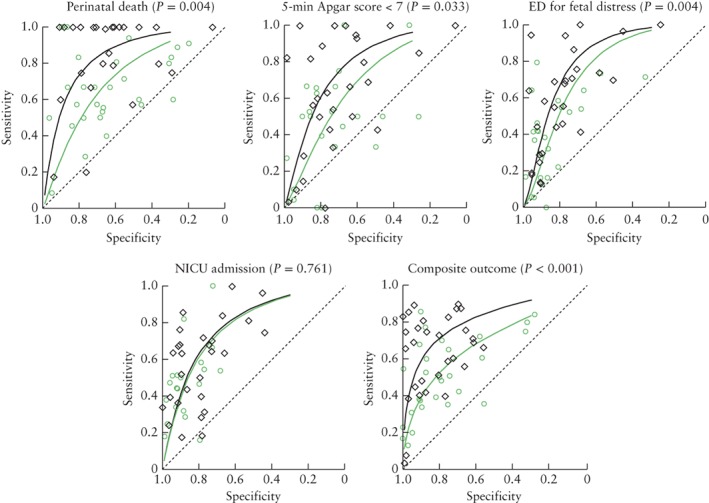
The search identified 4693 articles, of which 128 studies (involving 47 748 women) were included. Risk of bias or suboptimal reporting was detected in 120/128 studies (94%) and substantial heterogeneity was found, which limited subgroup analyses for fetal growth and gestational age. A large variation was observed in reported sensitivities and specificities, and in thresholds used. CPR outperformed UA Doppler in the prediction of composite adverse outcome (as defined in the included studies) (P < 0.001) and emergency delivery for fetal distress (P = 0.003), but was comparable to UA Doppler for the other outcomes. MCA Doppler performed significantly worse than did UA Doppler in the prediction of low Apgar score (P = 0.017) and emergency delivery for fetal distress (P = 0.034). CPR outperformed MCA Doppler in the prediction of composite adverse outcome (P < 0.001) and emergency delivery for fetal distress (P = 0.013).
Calculating the CPR with MCA Doppler can add value to UA Doppler assessment in the prediction of adverse perinatal outcome in women with a singleton pregnancy. However, it is unclear to which subgroup of pregnant women this applies. The effectiveness of the CPR in guiding clinical management needs to be evaluated in clinical trials. © 2017 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
多普勒超声评估脑胎盘比(CPR)和大脑中动脉(MCA)广泛用作脐带动脉(UA)多普勒的辅助手段,以识别有不良围产儿结局风险的胎儿。然而,报告的准确性估计差异很大。本研究旨在系统回顾 CPR 和 MCA 多普勒在预测不良围产儿结局方面的预测准确性,并将其与 UA 多普勒进行比较,以确定 CPR 和 MCA 多普勒评估是否对 UA 多普勒具有附加价值。
从建库到 2016 年 6 月,我们在 PubMed、EMBASE、Cochrane 图书馆和 ClinicalTrials.gov 上搜索了关于 UA 多普勒与 CPR 和/或 MCA 多普勒在预测各种风险特征的单胎妊娠不良围产儿结局方面的预测准确性的研究。使用 QUADAS-2(诊断准确性研究的质量评估-2)工具评估偏倚风险和适用性问题。对多种不良围产儿结局进行了荟萃分析。使用分层综合受试者工作特征荟萃回归模型,间接比较了 CPR 与 MCA 多普勒的预测准确性,并直接比较了 CPR 和 MCA 多普勒与 UA 多普勒的预测准确性。
搜索共确定了 4693 篇文章,其中包括 128 项研究(涉及 47748 名女性)。128 项研究中有 120 项(94%)存在偏倚或报告不充分,且存在很大的异质性,限制了对胎儿生长和胎龄的亚组分析。报告的敏感度和特异度以及使用的阈值差异很大。CPR 在预测复合不良结局(纳入研究中定义)(P<0.001)和因胎儿窘迫行紧急分娩(P=0.003)方面优于 UA 多普勒,但在其他结局方面与 UA 多普勒相当。MCA 多普勒在预测低 Apgar 评分(P=0.017)和因胎儿窘迫行紧急分娩(P=0.034)方面的表现明显劣于 UA 多普勒。CPR 在预测复合不良结局(P<0.001)和因胎儿窘迫行紧急分娩(P=0.013)方面优于 MCA 多普勒。
计算 CPR 时联合 MCA 多普勒可增加 UA 多普勒评估在预测单胎妊娠不良围产儿结局方面的价值。然而,尚不清楚这适用于哪些孕妇亚组。CPR 在指导临床管理中的有效性需要在临床试验中进行评估。© 2017 作者。《超声医学杂志》由约翰威立父子公司出版,代表国际妇产科超声学会。