Kotecha Dipak, Calvert Melanie, Deeks Jonathan J, Griffith Michael, Kirchhof Paulus, Lip Gregory Yh, Mehta Samir, Slinn Gemma, Stanbury Mary, Steeds Richard P, Townend Jonathan N
Institute of Cardiovascular Sciences, University of Birmingham, Birmingham, UK.
Cardiology, University Hospitals Birmingham NHS Trust, Birmingham, UK.
BMJ Open. 2017 Jul 20;7(7):e015099. doi: 10.1136/bmjopen-2016-015099.
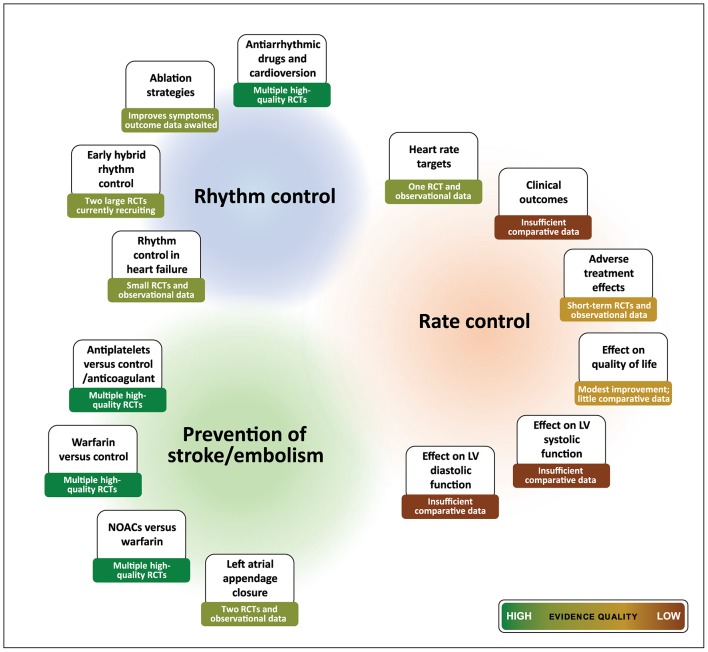
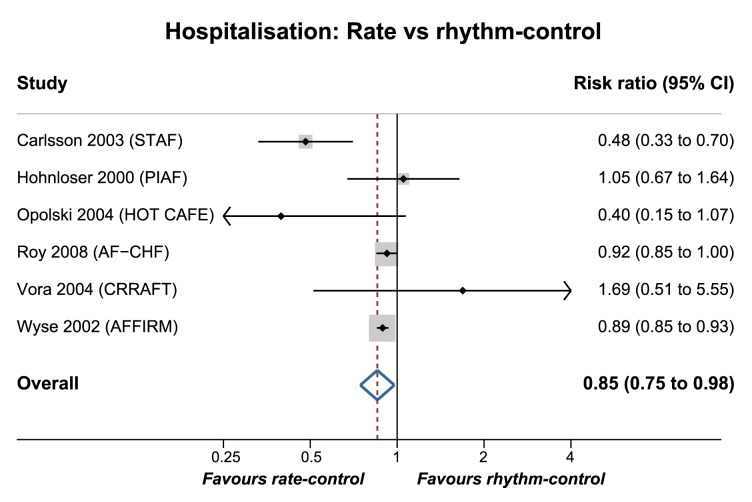
Atrial fibrillation (AF) is common and causes impaired quality of life, an increased risk of stroke and death as well as frequent hospital admissions. The majority of patients with AF require control of heart rate. In this article , we summarise the limited evidence from clinical trials that guides prescription, and present the rationale and protocol for a new randomised trial. As rate control has not yet been shown to reduce mortality, there is a clear need to compare the impact of therapy on quality of life, cardiac function and exercise capacity. Such a trial should concentrate on the long-term effects of treatment in the largest proportion of patients with AF, those with symptomatic permanent AF, with the aim of improving patient well-being.
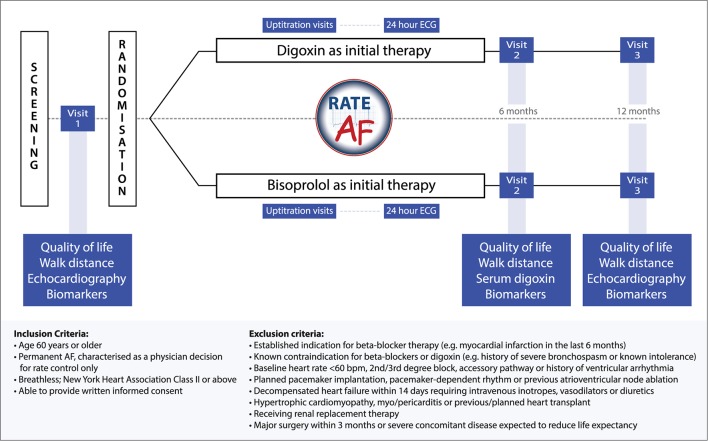
The RAte control Therapy Evaluation in permanent Atrial Fibrillation (RATE-AF) trial will enrol 160 participants with a prospective, randomised, open-label, blinded end point design comparing initial rate control with digoxin or bisoprolol. This will be the first head-to-head randomised trial of digoxin and beta-blockers in AF.
Recruited patients will be aged ≥60 years with permanent AF and symptoms of breathlessness (equivalent to New York Heart Association class II or above), with few exclusion criteria to maximise generalisability to routine clinical practice.
The primary outcome is patient-reported quality of life, with secondary outcomes including echocardiographic ventricular function, exercise capacity and biomarkers of cellular and clinical response. Follow-up will occur at 6 and 12 months, with feasibility components to inform the design of a future trial powered to detect a difference in hospital admission. The RATE-AF trial will underpin an integrated approach to management including biomarkers, functions and symptoms that will guide future research into optimal, personalised rate control in patients with AF.
East Midlands-Derby Research Ethics Committee (16/EM/0178); peer-reviewed publications.
Clinicaltrials.gov: NCT02391337; ISRCTN: 95259705. Pre-results.
心房颤动(AF)很常见,会导致生活质量下降、中风和死亡风险增加以及频繁住院。大多数房颤患者需要控制心率。在本文中,我们总结了临床试验中指导用药的有限证据,并介绍了一项新的随机试验的基本原理和方案。由于尚未证明心率控制能降低死亡率,因此显然有必要比较治疗对生活质量、心功能和运动能力的影响。这样一项试验应专注于治疗对最大比例房颤患者(即有症状的永久性房颤患者)的长期影响,旨在改善患者的健康状况。
永久性心房颤动心率控制治疗评估(RATE-AF)试验将招募160名参与者,采用前瞻性、随机、开放标签、盲终点设计,比较地高辛或比索洛尔的初始心率控制效果。这将是第一项关于地高辛和β受体阻滞剂在房颤治疗中直接对比的随机试验。
招募的患者年龄≥60岁,患有永久性房颤且有呼吸困难症状(相当于纽约心脏协会II级或以上),排除标准很少,以最大限度地提高对常规临床实践的适用性。
主要观察指标是患者报告的生活质量,次要观察指标包括超声心动图心室功能、运动能力以及细胞和临床反应的生物标志物。随访将在6个月和12个月时进行,还有可行性部分,为未来一项有足够效力检测住院差异的试验设计提供信息。RATE-AF试验将支持一种综合管理方法(包括生物标志物、功能和症状),这将指导未来对房颤患者进行最佳、个性化心率控制的研究。
东米德兰兹-德比研究伦理委员会(16/EM/0178);同行评审出版物。
Clinicaltrials.gov:NCT02391337;ISRCTN:95259705。预结果。