Acedillo Rey R, Wald Ron, McArthur Eric, Nash Danielle Marie, Silver Samuel A, James Matthew T, Schull Michael J, Siew Edward D, Matheny Michael E, House Andrew A, Garg Amit X
Division of Nephrology, Department of Medicine, London Health Sciences Centre, London, Ontario, Canada.
Department of Epidemiology and Biostatistics, Western University, London, Ontario, Canada.
Clin J Am Soc Nephrol. 2017 Aug 7;12(8):1215-1225. doi: 10.2215/CJN.10431016. Epub 2017 Jul 20.
Patients discharged home from an emergency department with AKI are not well described. This study describes their characteristics and outcomes and compares these outcomes to two referent groups.
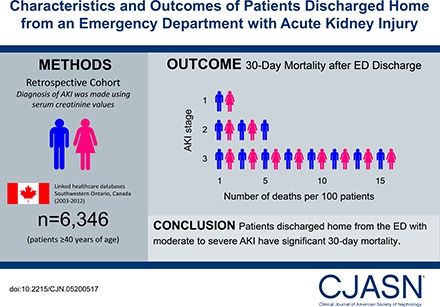
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We conducted a population-based retrospective cohort study in Ontario, Canada from 2003 to 2012 of 6346 patients aged ≥40 years who were discharged from the emergency department with AKI (defined using serum creatinine values). We analyzed the risk of all-cause mortality, receipt of acute dialysis, and hospitalization within 30 days after discharge. We used propensity score methods to compare all-cause mortality to two referent groups. We matched 4379 discharged patients to 4379 patients who were hospitalized from the emergency department with similar AKI stage. We also matched 6188 discharged patients to 6188 patients who were discharged home from the emergency department with no AKI.
There were 6346 emergency department discharges with AKI. The mean age was 69 years and 6012 (95%) had stage 1, 290 (5%) had stage 2, and 44 (0.7%) had stage 3 AKI. Within 30 days, 149 (2%) (AKI stage 1: 127 [2%]; stage 2: 15 [5%]; stage 3: seven [16%]) died, 22 (0.3%) received acute dialysis, and 1032 (16%) were hospitalized. An emergency department discharge versus hospitalization with AKI was associated with lower mortality (3% versus 12%; relative risk, 0.3; 95% confidence interval, 0.2 to 0.3). An emergency department discharge with AKI versus no AKI was associated with higher mortality (2% versus 1%; relative risk, 1.6; 95% confidence interval, 1.2 to 2.0).
Patients discharged home from the emergency department with AKI are at risk of poor 30-day outcomes. A better understanding of care in this at-risk population is warranted, as are testing strategies to improve care.
关于急性肾损伤(AKI)患者从急诊科出院后回家的情况,目前尚无充分描述。本研究描述了这些患者的特征和结局,并将这些结局与两个参照组进行比较。
设计、地点、参与者及测量方法:我们在加拿大安大略省进行了一项基于人群的回顾性队列研究,研究对象为2003年至2012年间6346名年龄≥40岁且从急诊科出院的AKI患者(根据血清肌酐值定义)。我们分析了出院后30天内全因死亡、接受急性透析和再次住院的风险。我们使用倾向评分方法将全因死亡率与两个参照组进行比较。我们将4379名出院患者与4379名因类似AKI分期从急诊科住院的患者进行匹配。我们还将6188名出院患者与6188名从急诊科出院且无AKI的患者进行匹配。
共有6346例从急诊科出院的AKI患者。平均年龄为69岁,6012例(95%)为1期,290例(5%)为2期,44例(0.7%)为3期AKI。在30天内,149例(2%)(1期AKI:127例[2%];2期:15例[5%];3期:7例[16%])死亡,22例(0.3%)接受急性透析,1032例(16%)再次住院。与因AKI住院相比,从急诊科出院与较低的死亡率相关(3%对12%;相对风险,0.3;95%置信区间,0.2至0.3)。与无AKI从急诊科出院相比,因AKI从急诊科出院与较高的死亡率相关(2%对1%;相对风险,1.6;95%置信区间,1.2至2.0)。
从急诊科出院回家的AKI患者有30天结局不良的风险。有必要更好地了解这一高危人群的护理情况,以及改善护理的测试策略。