Hobbs Helen, Bassett Paul, Wheeler Toby, Bedford Michael, Irving Jean, Stevens Paul E, Farmer Christopher K T
East Kent University Hospitals NHS Foundation Trust, Kidney Kent Research Group, Kent Kidney Care Centre, Kent and Canterbury Hospital, Ethelbert Road, Canterbury, Kent CT1 3NG, England.
BMC Nephrol. 2014 Dec 22;15:206. doi: 10.1186/1471-2369-15-206.
The significant impact Acute Kidney Injury (AKI) has on patient morbidity and mortality emphasizes the need for early recognition and effective treatment. AKI presenting to or occurring during hospitalisation has been widely studied but little is known about the incidence and outcomes of patients experiencing acute elevations in serum creatinine in the primary care setting where people are not subsequently admitted to hospital. The aim of this study was to define this incidence and explore its impact on mortality.
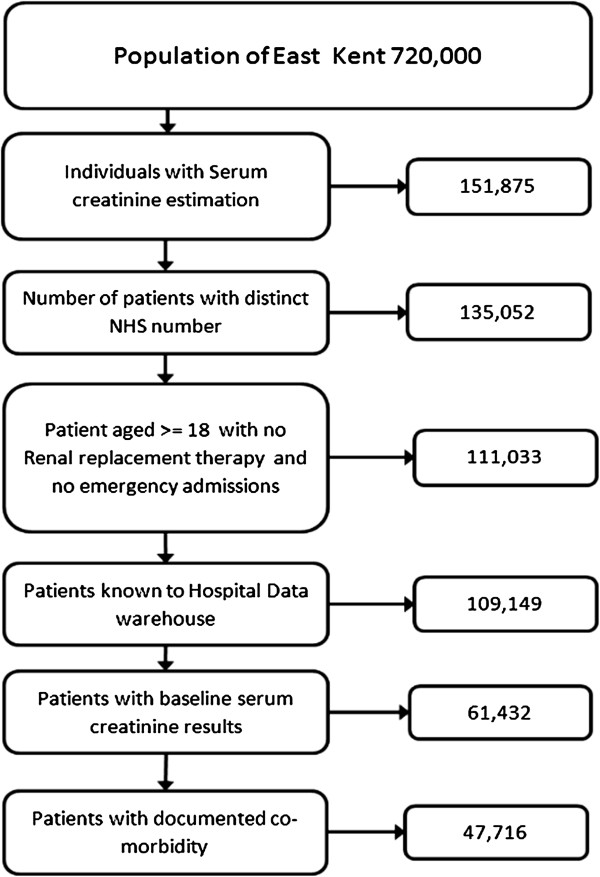
The study cohort was identified by using hospital data bases over a six month period.
People with a serum creatinine request during the study period, 18 or over and not on renal replacement therapy.The patients were stratified by a rise in serum creatinine corresponding to the Acute Kidney Injury Network (AKIN) criteria for comparison purposes. Descriptive and survival data were then analysed.Ethical approval was granted from National Research Ethics Service (NRES) Committee South East Coast and from the National Information Governance Board.
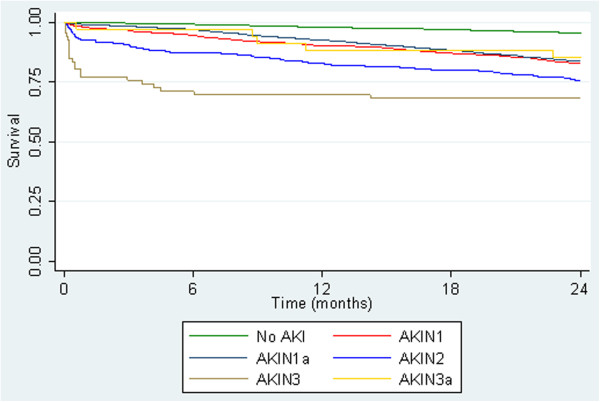
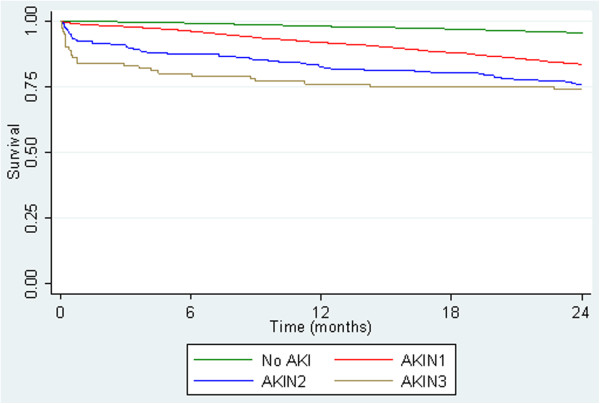
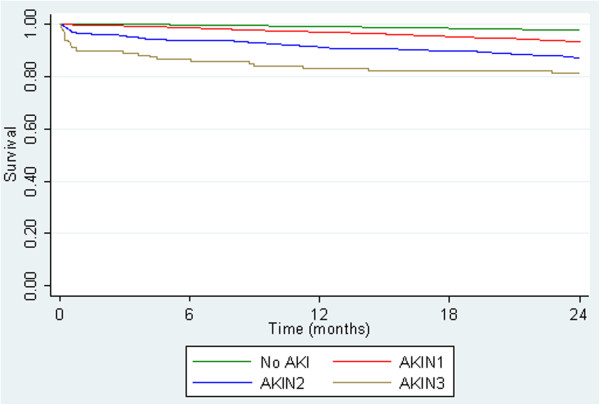
The total study population was 61,432. 57,300 subjects with 'no AKI', mean age 64.The number (mean age) of acute serum creatinine rises overall were, 'AKI 1' 3,798 (72), 'AKI 2' 232 (73), and 'AKI 3' 102 (68) which equates to an overall incidence of 14,192 pmp/year (adult). Unadjusted 30 day survival was 99.9% in subjects with 'no AKI', compared to 98.6%, 90.1% and 82.3% in those with 'AKI 1', 'AKI 2' and 'AKI 3' respectively. After multivariable analysis adjusting for age, gender, baseline kidney function and co-morbidity the odds ratio of 30 day mortality was 5.3 (95% CI 3.6, 7.7), 36.8 (95% CI 21.6, 62.7) and 123 (95% CI 64.8, 235) respectively, compared to those without acute serum creatinine rises as defined.
People who develop acute elevations of serum creatinine in primary care without being admitted to hospital have significantly worse outcomes than those with stable kidney function.
急性肾损伤(AKI)对患者发病率和死亡率有重大影响,这凸显了早期识别和有效治疗的必要性。在住院期间出现或发生的AKI已得到广泛研究,但对于在初级保健环境中血清肌酐急性升高且随后未住院的患者的发病率和预后知之甚少。本研究的目的是确定这一发病率并探讨其对死亡率的影响。
通过使用医院数据库在六个月期间确定研究队列。
在研究期间有血清肌酐检测需求、年龄在18岁及以上且未接受肾脏替代治疗的人群。为了进行比较,根据急性肾损伤网络(AKIN)标准将患者按血清肌酐升高情况进行分层。然后分析描述性和生存数据。获得了国家研究伦理服务(NRES)委员会东南海岸分会和国家信息治理委员会的伦理批准。
总研究人群为61432人。57300名“无AKI”受试者,平均年龄64岁。血清肌酐急性升高的总体人数(平均年龄)分别为:“AKI 1”3798人(72岁)、“AKI 2”232人(73岁)和“AKI 3”102人(68岁),相当于成人总体发病率为每年14192例/百万人口。“无AKI”受试者的未调整30天生存率为99.9%,而“AKI 1”、“AKI 2”和“AKI 3”受试者的相应生存率分别为98.6%、90.1%和82.3%。在对年龄、性别、基线肾功能和合并症进行多变量分析后,与未出现所定义的血清肌酐急性升高情况的受试者相比,30天死亡率的优势比分别为5.3(95%置信区间3.6, 7.7)、36.8(95%置信区间21.6, 62.7)和123(95%置信区间64.8, 235)。
在初级保健中出现血清肌酐急性升高但未住院的患者,其预后明显比肾功能稳定的患者差。