Kawashima Chika, Matsuzawa Yasushi, Akiyama Eiichi, Konishi Masaaki, Suzuki Hiroyuki, Hashiba Katsutaka, Ebina Toshiaki, Kosuge Masami, Hibi Kiyoshi, Tsukahara Kengo, Iwahashi Noriaki, Maejima Nobuhiko, Sakamaki Kentaro, Umemura Satoshi, Kimura Kazuo, Tamura Kouichi
Division of Cardiology, Yokohama City University Medical Center, Yokohama, Japan.
Division of Cardiology, Yokohama City University Medical Center, Yokohama, Japan
J Am Heart Assoc. 2017 Jul 22;6(7):e005463. doi: 10.1161/JAHA.116.005463.
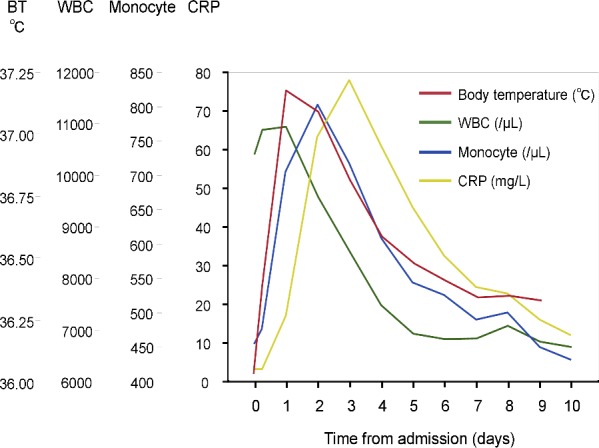
The biphasic inflammation after ST-segment elevation myocardial infarction (STEMI) plays an important role in myocardial healing and progression of systemic atherosclerosis. The purpose of this study is to investigate the impact of fever during the first and second phases of post-STEMI inflammation on long-term cardiac outcomes.
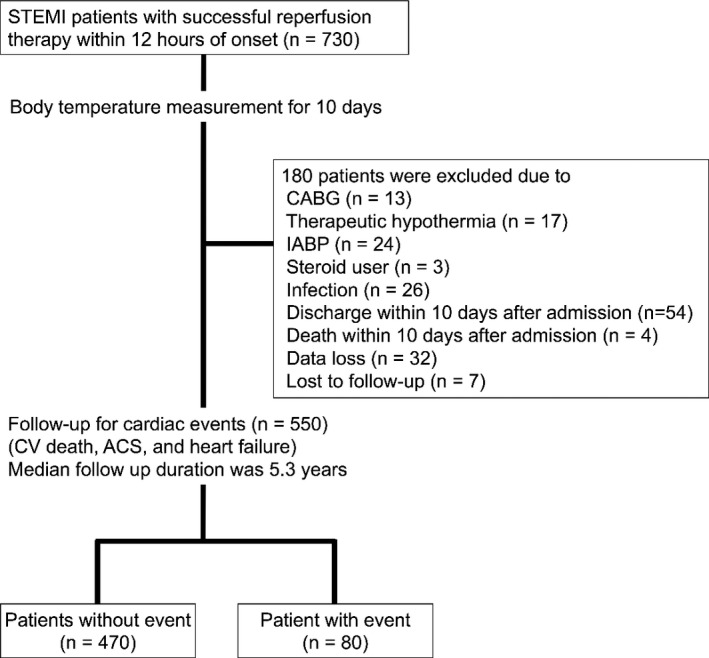
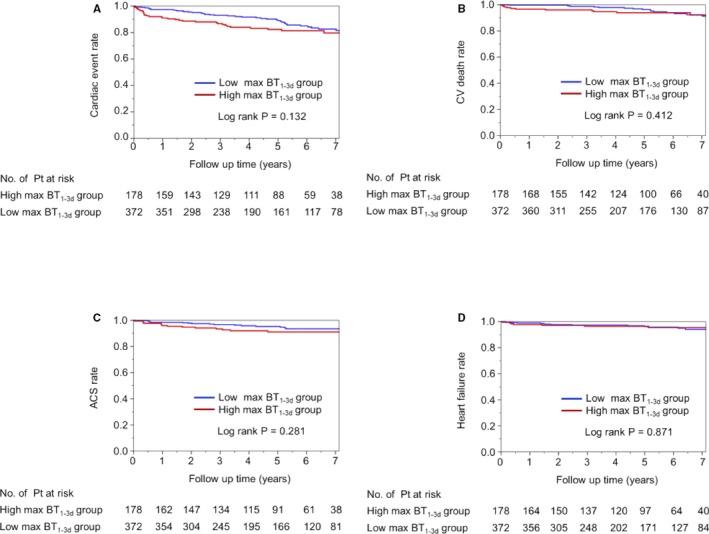
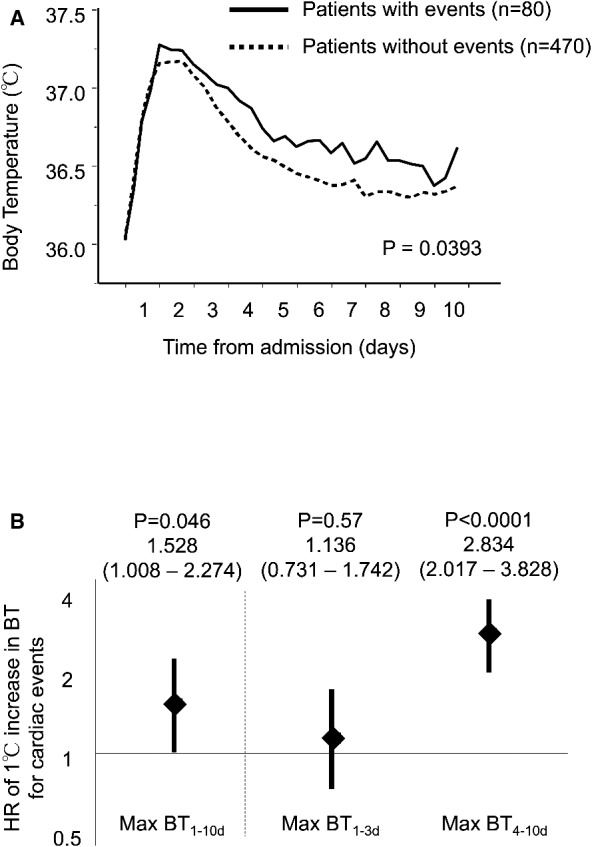
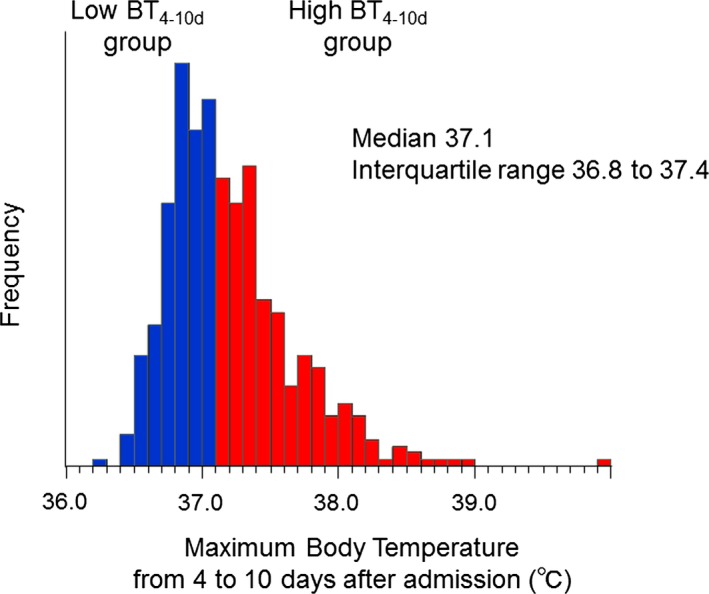
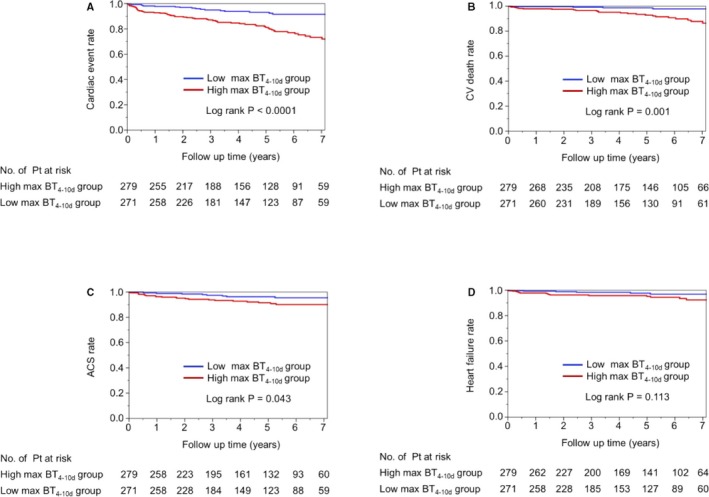
A total of 550 patients with STEMI were enrolled in this study. Axillary body temperature (BT) was measured and maximum BTs were determined for the first (within 3 days: max-BT) and second (from 4 to 10 days after admission: max-BT) phases, respectively. Patients were followed for cardiac events (cardiovascular death, acute coronary syndrome, and rehospitalization for heart failure) for a median 5.3 years. During the follow-up period, 80 patients experienced cardiac events. A high max-BT was strongly associated with long-term cardiac events (hazard ratio, 95% CI) for a 1°C increase in the max-BT: 2.834 (2.017-3.828), <0.0001, whereas the max-BT was not associated with cardiac events (1.136 [0.731-1.742], =0.57). Even after adjustment for coronary risk factors, estimated glomerular filtration rate, infarct size, pericardial effusion, and medications on discharge, fever during the second phase (max-BT ≥37.1°C) was significantly associated with future cardiac events (hazard ratio [95% CI] 2.900 [1.710-5.143], <0.0001).
Fever during the second phase but not the first phase of post-STEMI inflammation was a strong associated factor with worse long-term cardiac outcomes in patients after STEMI, suggesting the need to consider the optimal timing for anti-inflammatory strategies after STEMI.
ST段抬高型心肌梗死(STEMI)后的双相炎症在心肌愈合和全身动脉粥样硬化进展中起重要作用。本研究旨在探讨STEMI后炎症第一阶段和第二阶段发热对长期心脏结局的影响。
本研究共纳入550例STEMI患者。测量腋温,并分别确定第一阶段(3天内:最高体温)和第二阶段(入院后4至10天:最高体温)的最高体温。对患者进行心脏事件(心血管死亡、急性冠状动脉综合征和因心力衰竭再次住院)随访,中位随访时间为5.3年。随访期间,80例患者发生心脏事件。最高体温每升高1°C,高最高体温与长期心脏事件密切相关(风险比,95%CI):2.834(2.017 - 3.828),<0.0001,而最高体温与心脏事件无关(1.136 [0.731 - 1.742],P = 0.57)。即使在调整了冠状动脉危险因素、估计肾小球滤过率、梗死面积、心包积液和出院时使用的药物后,第二阶段发热(最高体温≥37.1°C)仍与未来心脏事件显著相关(风险比[95%CI] 2.900 [1.710 - 5.143],<0.0001)。
STEMI后炎症第二阶段而非第一阶段的发热是STEMI患者长期心脏结局较差的强相关因素,提示需要考虑STEMI后抗炎策略的最佳时机。