Churpek Matthew M, Snyder Ashley, Sokol Sarah, Pettit Natasha N, Edelson Dana P
1Department of Medicine, University of Chicago, Chicago, IL. 2Department of Pharmacy, University of Chicago, Chicago, IL.
Crit Care Med. 2017 Nov;45(11):1805-1812. doi: 10.1097/CCM.0000000000002648.
Studies in sepsis are limited by heterogeneity regarding what constitutes suspicion of infection. We sought to compare potential suspicion criteria using antibiotic and culture order combinations in terms of patient characteristics and outcomes. We further sought to determine the impact of differing criteria on the accuracy of sepsis screening tools and early warning scores.
Observational cohort study.
Academic center from November 2008 to January 2016.
Hospitalized patients outside the ICU.
None.
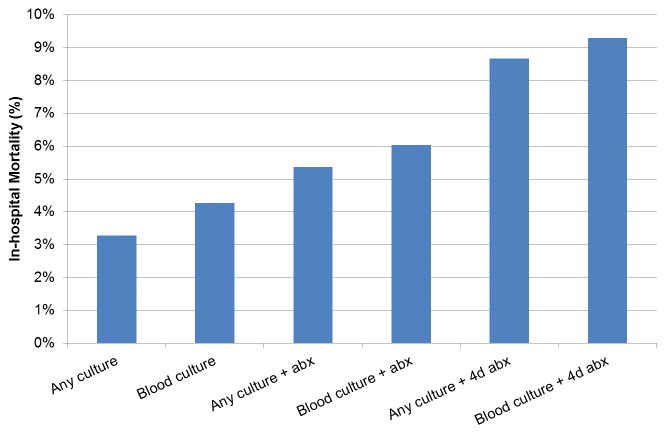
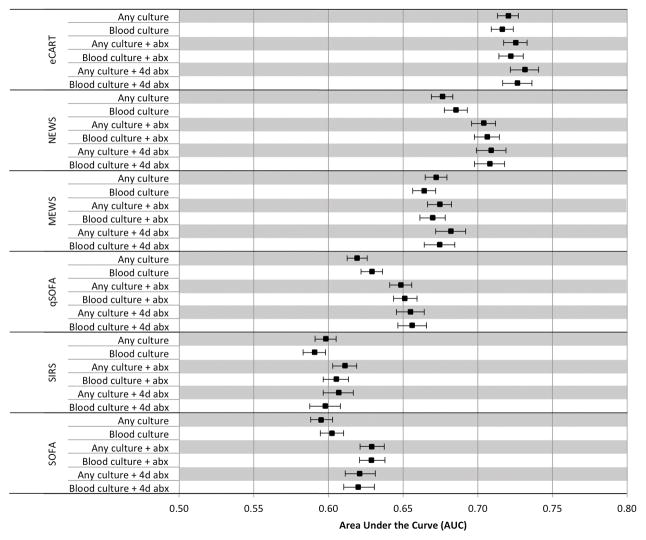
Six criteria were investigated: 1) any culture, 2) blood culture, 3) any culture plus IV antibiotics, 4) blood culture plus IV antibiotics, 5) any culture plus IV antibiotics for at least 4 of 7 days, and 6) blood culture plus IV antibiotics for at least 4 of 7 days. Accuracy of the quick Sepsis-related Organ Failure Assessment score, Sepsis-related Organ Failure Assessment score, systemic inflammatory response syndrome criteria, the National and Modified Early Warning Score, and the electronic Cardiac Arrest Risk Triage score were calculated for predicting ICU transfer or death within 48 hours of meeting suspicion criteria. A total of 53,849 patients met at least one infection criteria. Mortality increased from 3% for group 1 to 9% for group 6 and percentage meeting Angus sepsis criteria increased from 20% to 40%. Across all criteria, score discrimination was lowest for systemic inflammatory response syndrome (median area under the receiver operating characteristic curve, 0.60) and Sepsis-related Organ Failure Assessment score (median area under the receiver operating characteristic curve, 0.62), intermediate for quick Sepsis-related Organ Failure Assessment (median area under the receiver operating characteristic curve, 0.65) and Modified Early Warning Score (median area under the receiver operating characteristic curve 0.67), and highest for National Early Warning Score (median area under the receiver operating characteristic curve 0.71) and electronic Cardiac Arrest Risk Triage (median area under the receiver operating characteristic curve 0.73).
The choice of criteria to define a potentially infected population significantly impacts prevalence of mortality but has little impact on accuracy. Systemic inflammatory response syndrome was the least predictive and electronic Cardiac Arrest Risk Triage the most predictive regardless of how infection was defined.
脓毒症研究因对感染疑似标准的定义存在异质性而受到限制。我们试图通过抗生素和培养医嘱组合来比较潜在的疑似标准,分析其患者特征和预后情况。我们还进一步试图确定不同标准对脓毒症筛查工具和早期预警评分准确性的影响。
观察性队列研究。
2008年11月至2016年1月期间的学术中心。
重症监护病房(ICU)以外的住院患者。
无。
研究了六种标准:1)任何培养;2)血培养;3)任何培养加静脉用抗生素;4)血培养加静脉用抗生素;5)任何培养加静脉用抗生素至少7天中的4天;6)血培养加静脉用抗生素至少7天中的4天。计算了快速脓毒症相关器官功能衰竭评估评分、脓毒症相关器官功能衰竭评估评分、全身炎症反应综合征标准、国家早期预警评分和改良早期预警评分以及电子心脏骤停风险分诊评分在达到疑似标准后48小时内预测转入ICU或死亡的准确性。共有53849名患者符合至少一项感染标准。死亡率从第1组的3%上升至第6组的9%,符合安格斯脓毒症标准的比例从20%增至40%。在所有标准中,全身炎症反应综合征的评分辨别力最低(受试者操作特征曲线下面积中位数为0.60),脓毒症相关器官功能衰竭评估评分次之(受试者操作特征曲线下面积中位数为0.62),快速脓毒症相关器官功能衰竭评估(受试者操作特征曲线下面积中位数为0.65)和改良早期预警评分居中(受试者操作特征曲线下面积中位数为0.67),国家早期预警评分最高(受试者操作特征曲线下面积中位数为0.71),电子心脏骤停风险分诊评分最高(受试者操作特征曲线下面积中位数为图0.73)。
定义潜在感染人群的标准选择对死亡率有显著影响,但对准确性影响不大。无论感染如何定义,全身炎症反应综合征的预测性最低,而电子心脏骤停风险分诊的预测性最高。