Department of Internal Medicine, Atrium Health Wake Forest Baptist, Winston-Salem, North Carolina.
Section of Pulmonology, Critical Care, Allergy and Immunologic Diseases, Atrium Health Wake Forest Baptist, Winston-Salem, North Carolina.
JAMA Netw Open. 2023 Aug 1;6(8):e2329729. doi: 10.1001/jamanetworkopen.2023.29729.
The Sepsis Prediction Model (SPM) is a proprietary decision support tool created by Epic Systems; it generates a predicting sepsis score (PSS). The model has not undergone validation against existing sepsis prediction tools, such as Systemic Inflammatory Response Syndrome (SIRS), Sequential Organ Failure Assessment (SOFA), or quick Sepsis-Related Organ Failure Asessement (qSOFA).
To assess the validity and timeliness of the SPM compared with SIRS, qSOFA, and SOFA.
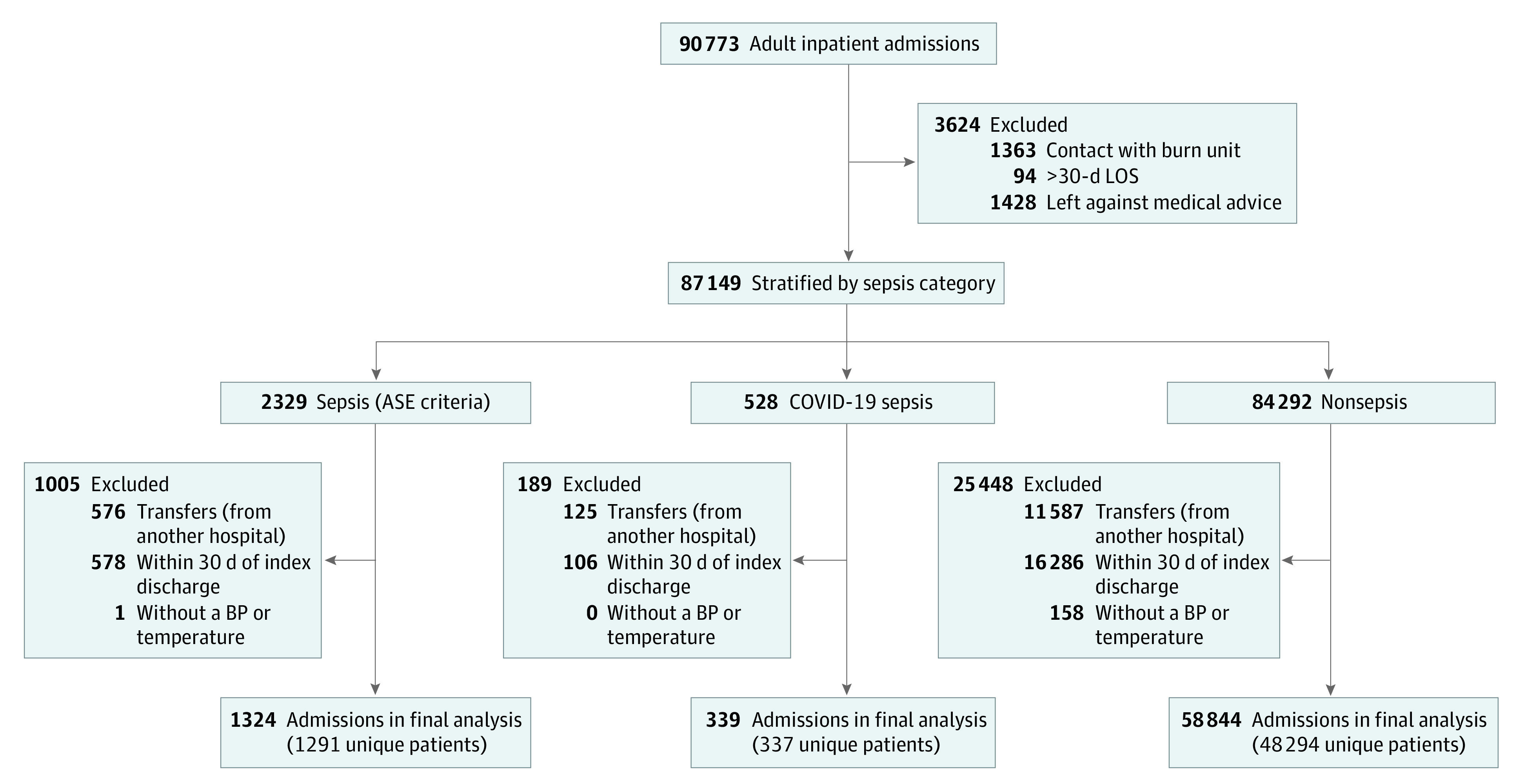
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study included all adults admitted to 5 acute care hospitals in a single US health system between June 5, 2019, and December 31, 2020. Data analysis was conducted from March 2021 to February 2023.
A sepsis event was defined as receipt of 4 or more days of antimicrobials, blood cultures collected within ±48 hours of initial antimicrobial, and at least 1 organ dysfunction as defined by the organ dysfunction criteria optimized for the electronic health record (eSOFA). Time zero was defined as 15 minutes prior to qualifying antimicrobial or blood culture order.
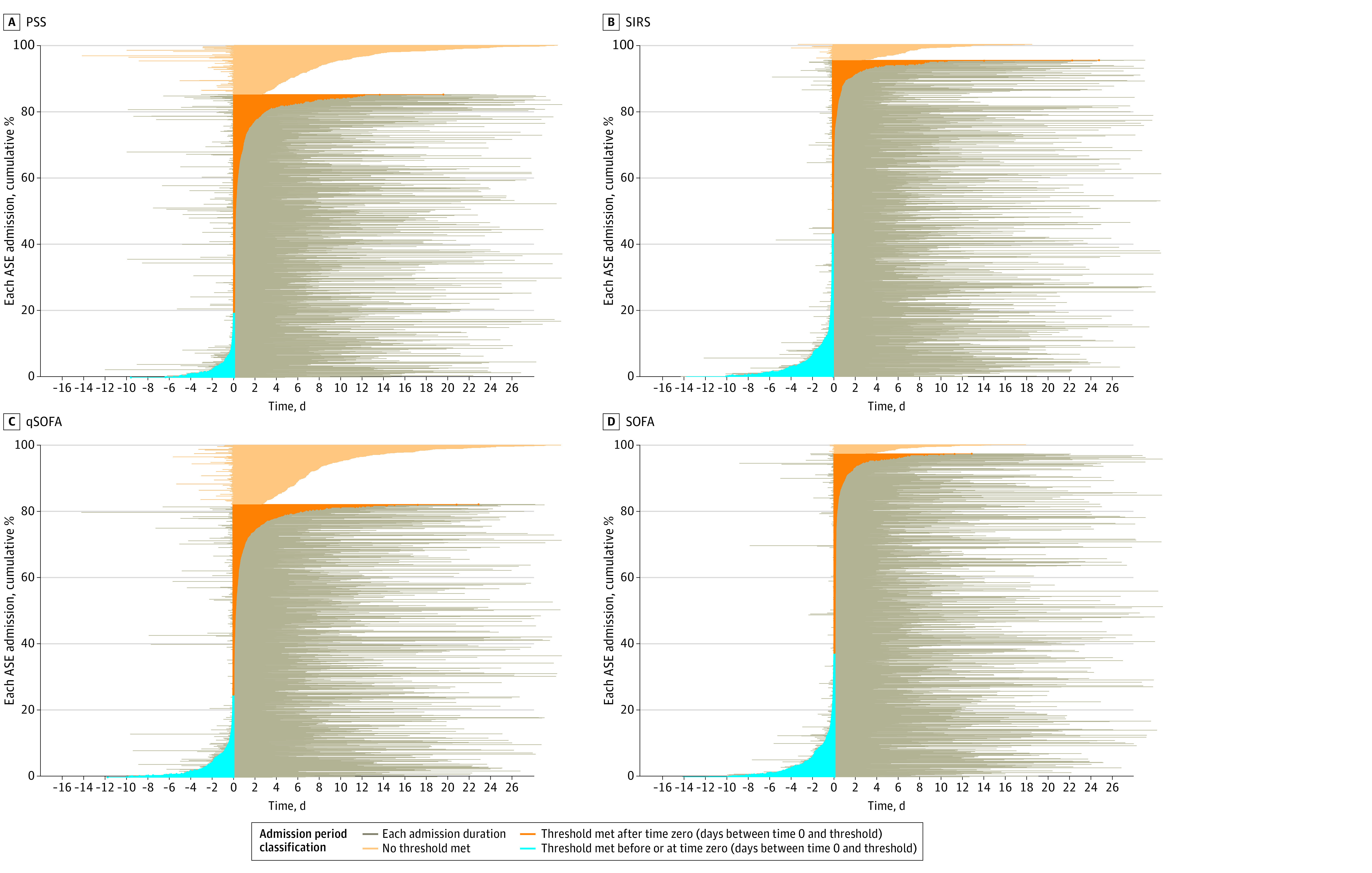
Of 60 507 total admissions, 1663 (2.7%) met sepsis criteria, with 1324 electronic health record-confirmed sepsis (699 [52.8%] male patients; 298 [22.5%] Black patients; 46 [3.5%] Hispanic/Latinx patients; 945 [71.4%] White patients), 339 COVID-19 sepsis (183 [54.0%] male patients; 98 [28.9%] Black patients; 36 [10.6%] Hispanic/Latinx patients; and 189 [55.8%] White patients), and 58 844 (97.3%; 26 632 [45.2%] male patients; 12 698 [21.6%] Black patients; 3367 [5.7%] Hispanic/Latinx patients; 40 491 White patients) did not meet sepsis criteria. The median (IQR) age was 63 (51 to 73) years for electronic health record-confirmed sepsis, 69 (60 to 77) years for COVID-19 sepsis, and 60 (42 to 72) years for nonsepsis admissions. Within the vendor recommended threshold PSS range of 5 to 8, PSS of 8 or greater had the highest balanced accuracy for classifying a sepsis admission at 0.79 (95% CI, 0.78 to 0.80). Change in SOFA score of 2 or more had the highest sensitivity, at 0.97 (95% CI, 0.97 to 0.98). At a PSS of 8 or greater, median (IQR) time to score positivity from time zero was 68.00 (6.75 to 605.75) minutes. For SIRS, qSOFA, and SOFA, median (IQR) time to score positivity was 7.00 (-105.00 to 08.00) minutes, 74.00 (-22.25 to 599.25) minutes, and 28.00 (-108.50 to 134.00) minutes, respectively.
In this cohort study of hospital admissions, balanced accuracy of the SPM outperformed other models at higher threshold PSS; however, application of the SPM in a clinical setting was limited by poor timeliness as a sepsis screening tool as compared to SIRS and SOFA.
Sepsis Prediction Model(SPM)是 Epic Systems 公司创建的专有决策支持工具;它生成一个预测败血症的分数(PSS)。该模型尚未经过与现有的败血症预测工具(如全身炎症反应综合征(SIRS)、序贯器官衰竭评估(SOFA)或快速相关器官衰竭评估(qSOFA))的验证。
评估 SPM 与 SIRS、qSOFA 和 SOFA 相比的有效性和及时性。
设计、地点和参与者:这项回顾性队列研究包括 2019 年 6 月 5 日至 2020 年 12 月 31 日期间在一个美国医疗系统的 5 家急性护理医院住院的所有成年人。数据分析于 2021 年 3 月至 2023 年 2 月进行。
败血症事件定义为接受 4 天以上的抗生素治疗、在开始使用抗生素的 ±48 小时内采集血液培养物,以及至少有一个器官功能障碍,符合电子健康记录优化的器官功能障碍标准(eSOFA)。零时定义为合格抗生素或血液培养物医嘱前 15 分钟。
在 60507 例总入院病例中,有 1663 例(2.7%)符合败血症标准,其中 1324 例电子健康记录确诊败血症(699 例[52.8%]男性患者;298 例[22.5%]黑人患者;46 例[3.5%]西班牙裔/拉丁裔患者;945 例[71.4%]白人患者),339 例 COVID-19 败血症(183 例[54.0%]男性患者;98 例[28.9%]黑人患者;36 例[10.6%]西班牙裔/拉丁裔患者;189 例[55.8%]白人患者),58844 例(97.3%;26632 例[45.2%]男性患者;12698 例[21.6%]黑人患者;3367 例[5.7%]西班牙裔/拉丁裔患者;40491 例白人患者)不符合败血症标准。电子健康记录确诊败血症的中位(IQR)年龄为 63(51 至 73)岁,COVID-19 败血症为 69(60 至 77)岁,非败血症入院为 60(42 至 72)岁。在供应商推荐的 5 至 8 分 PSS 范围内,8 分或更高的 PSS 对分类败血症入院的平衡准确性最高,为 0.79(95%CI,0.78 至 0.80)。SOFA 评分增加 2 分具有最高的敏感性,为 0.97(95%CI,0.97 至 0.98)。在 PSS 为 8 或更高的情况下,从零时到评分阳性的中位数(IQR)时间为 68.00(6.75 至 605.75)分钟。对于 SIRS、qSOFA 和 SOFA,评分阳性的中位数(IQR)时间分别为 7.00(-105.00 至 08.00)分钟、74.00(-22.25 至 599.25)分钟和 28.00(-108.50 至 134.00)分钟。
在这项医院入院队列研究中,SPM 的平衡准确性优于其他模型在较高的阈值 PSS 下的准确性;然而,与 SIRS 和 SOFA 相比,SPM 在临床环境中的应用受到较差的及时性的限制,作为一种败血症筛查工具。