Rava Paul, Rosenberg Jennifer, Jamorabo Daniel, Sioshansi Shirin, DiPetrillo Thomas, Wazer David E, Hepel Jaroslaw
Department of Radiation Oncology, University of Massachusetts, Worcester, Massachusetts.
Department of Radiation Oncology, Pennsylvania State University, Hershey, Pennsylvania.
Adv Radiat Oncol. 2016 Jun 23;1(3):141-147. doi: 10.1016/j.adro.2016.06.002. eCollection 2016 Jul-Sep.
Our objective was to report safety and efficacy of stereotactic radiosurgery (SRS) to the surgical bed following resection of brain metastases.
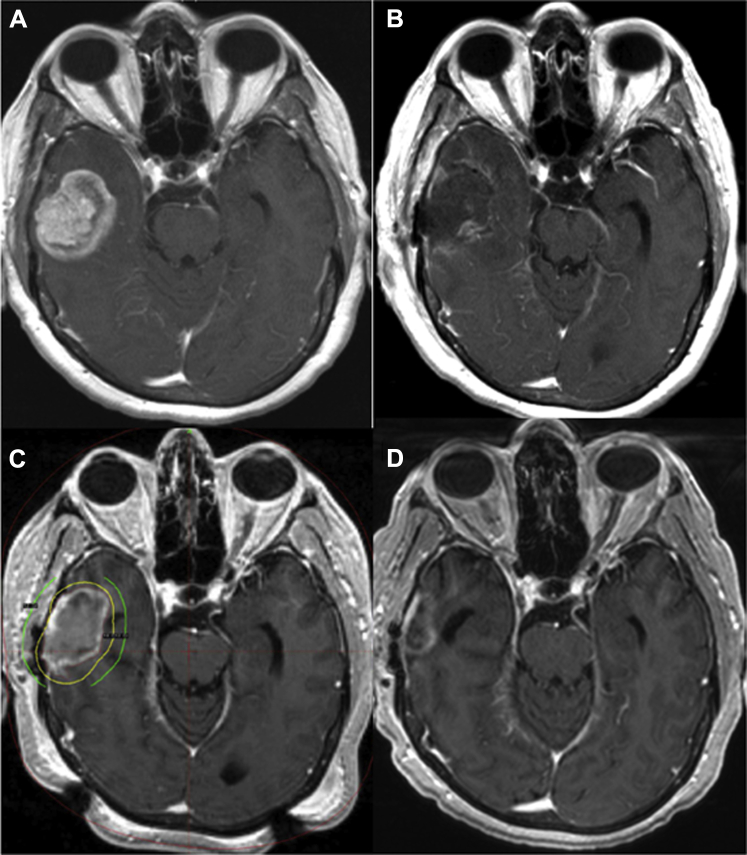
Eighty-seven consecutive patients who underwent cavity-directed SRS to the operative bed for the treatment of brain metastases between 2002 and 2010 were evaluated. SRS required a gadolinium-enhanced, high-resolution, T1-weighted magnetic resonance imaging for tumor targeting and delivered a median dose of 18 Gy (14-22 Gy) prescribed to encompass the entire resection cavity. Whole brain irradiation was reserved for salvage. Patients were followed every 3 months with clinical examination and magnetic resonance imaging. Overall survival, local and regional recurrence, and factors affecting these outcomes were evaluated using Kaplan-Meier and log-rank analyses.
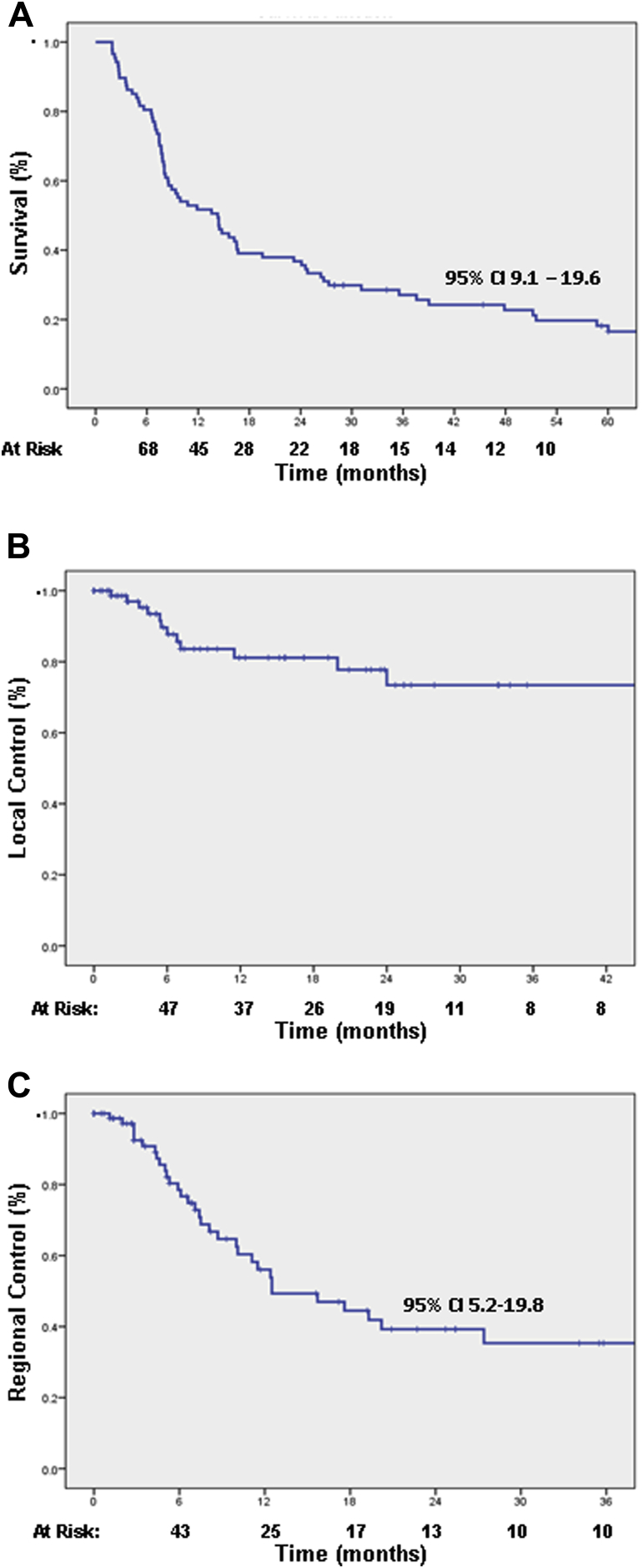
The median imaging follow-up was 7.1 months, with >40% of patients having imaging for ≥1 year. Local control at 1 and 2 years was 82% and 75%, respectively. Cavity recurrence was more common with a tumor diameter >3 cm ( < .020) or resection cavity volume >14 mL ( < .050). One-year local control for tumors <2 cm, 2 cm to 3 cm, and >3 cm were 100%, 86%, and 72%, respectively. Neither subtotal resection nor target margins >2 mm to 3 mm affected local control. The median overall survival was 14.3 months with actuarial 5-year survival of 20%. Actuarial regional central nervous system recurrence was 44% at 1 year. On univariate analysis, only the presence of extracranial disease was associated with survival ( < .001) and central nervous system failure ( < .030).
Excellent local control is achievable with cavity-directed SRS in well-selected patients, particularly for lesions with diameter <3 cm and resection cavity volumes <14 mL. Long-term survival is possible for select patients.
我们的目的是报告脑转移瘤切除术后对手术床进行立体定向放射外科治疗(SRS)的安全性和有效性。
对2002年至2010年间连续87例因脑转移瘤接受手术床定向SRS治疗的患者进行评估。SRS需要钆增强的高分辨率T1加权磁共振成像来靶向肿瘤,中位剂量为18 Gy(14 - 22 Gy),规定剂量覆盖整个切除腔。全脑照射留作挽救治疗。患者每3个月进行一次临床检查和磁共振成像随访。使用Kaplan-Meier和对数秩分析评估总生存期、局部和区域复发情况以及影响这些结果的因素。
影像学随访的中位时间为7.1个月,超过40%的患者进行了≥1年的影像学检查。1年和2年的局部控制率分别为82%和75%。肿瘤直径>3 cm(P<0.020)或切除腔体积>14 mL(P<0.050)时,腔隙复发更为常见。直径<2 cm、2 cm至3 cm和>3 cm的肿瘤1年局部控制率分别为100%、86%和72%。次全切除和靶边缘>2 mm至3 mm均不影响局部控制。中位总生存期为14.3个月,5年精算生存率为20%。1年时中枢神经系统区域精算复发率为44%。单因素分析显示只有存在颅外疾病与生存期(P<0.001)和中枢神经系统衰竭(P<0.030)相关。
对于精心挑选的患者,通过手术床定向SRS可实现出色的局部控制,尤其是对于直径<3 cm且切除腔体积<14 mL的病变。部分患者有可能实现长期生存。