Youland Ryan S, Packard Ann T, Blanchard Miran J, Arnett Andrea L, Wiseman Gregory A, Kottschade Lisa A, Dronca Roxana S, Markovic Svetomir N, Olivier Kenneth R, Park Sean S
Department of Radiation Oncology, Mayo Clinic, Rochester, Minnesota.
Division of Nuclear Medicine, Mayo Clinic, Rochester, Minnesota.
Adv Radiat Oncol. 2017 Feb 24;2(2):204-210. doi: 10.1016/j.adro.2017.02.003. eCollection 2017 Apr-Jun.
Clinical data that support stereotactic body radiation therapy (SBRT) metastatic malignant melanoma (MM) are limited. Furthermore, functional imaging with 18F-fludeoxyglucose positron emission tomography (PET) may offer a more accurate post-SBRT assessment. Therefore, we assessed the clinical outcomes and metabolic response of metastatic MM after SBRT.
Patients with MM who were treated with SBRT and had pre- and post-PET scans (>1) were included in this study. A total of 390 pre- and post-SBRT PET/computed tomography (CT) scans for 80 metastases were analyzed. The PET metabolic response was evaluated per the PET Response Criteria in Solid Tumors (PERCIST), version 1.0, criteria. Single-fraction equivalent dose (SFED) was calculated as per the standard. The Kaplan-Meier method was used for estimates of overall survival (OS) and progression-free survival. The cumulative incidence method was used to estimate metastasis control (MC). A Wilcoxon test was used to compare survival estimates. The prognostic factors for MC and OS were assessed using the Cox proportional hazards model, and the Likelihood Ratio was also used for comparisons between groups.
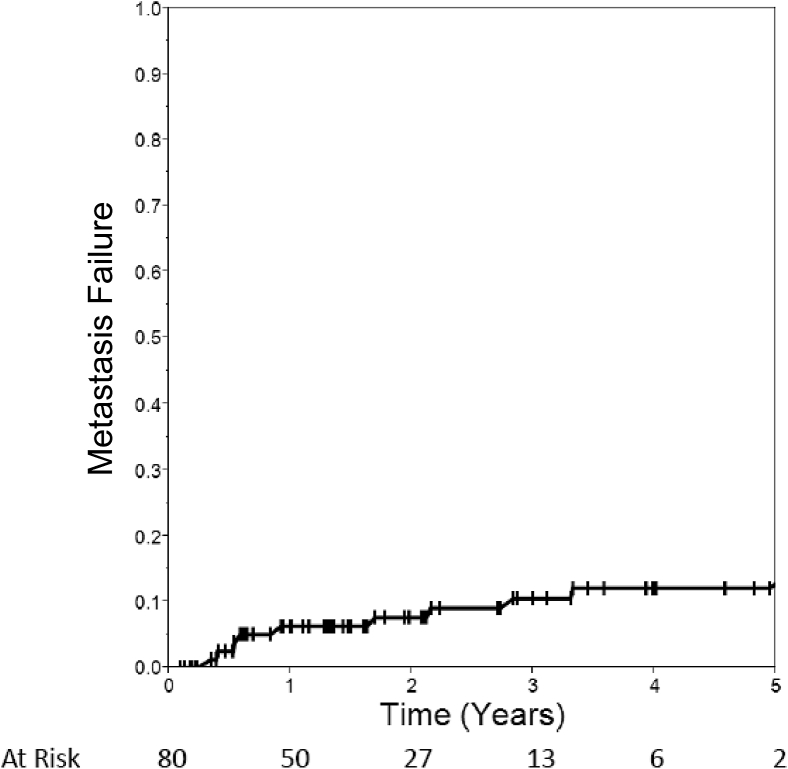
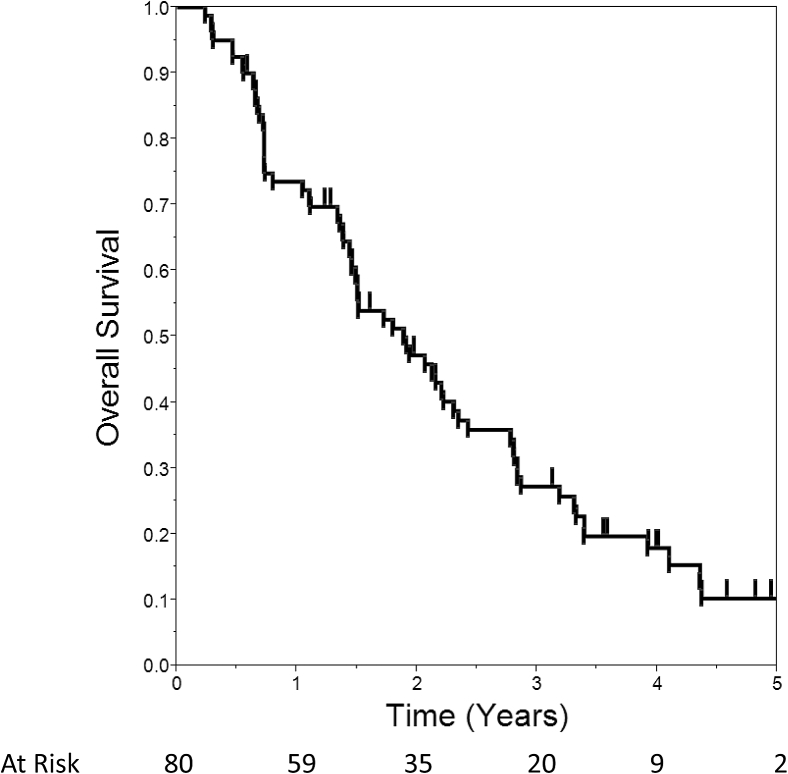
A median of 6 PET scans (range, 2-6 scans) was evaluated for each metastasis. The median SFED was 42.8 Gy (range, 18-56.4 Gy) and the median biologically effective dose was 254.4 Gy (range, 100.8-540 Gy). Twenty percent of patients received chemotherapy and 59% received immunotherapy: granulocyte-macrophage colony-stimulating factor (64%) and ipilimumab (34%). MC was 94% and 90% at 1 year and 3 years, respectively. The OS was 74% and 27% and 1 year and 3 years, respectively. Complete response was achieved in 90% at a median of 2.8 months (range, 0.4-25.2 months). SFED >24 Gy correlated with improved MC (93% vs 75%, = .01). Acute and late grade 3+ toxicities were 4% and 11%, respectively, with no grade 5 toxicity.
Post-SBRT PET/CT for extracranial metastatic MM resulted in high rates of complete response at a median of 2.8 months, and durable MC was achieved with SFED >24 Gy. SBRT, in addition to surgery and ablation, should be discussed with patients with MM, especially those with oligometastases.
支持立体定向体部放射治疗(SBRT)用于转移性恶性黑色素瘤(MM)的临床数据有限。此外,18F-氟脱氧葡萄糖正电子发射断层扫描(PET)功能成像可能提供更准确的SBRT后评估。因此,我们评估了SBRT后转移性MM的临床结局和代谢反应。
本研究纳入接受SBRT治疗且有PET扫描前后(>1次)的MM患者。共分析了80个转移灶的390次SBRT前后PET/计算机断层扫描(CT)。根据实体瘤PET反应标准(PERCIST)1.0版标准评估PET代谢反应。按标准计算单分次等效剂量(SFED)。采用Kaplan-Meier法估计总生存期(OS)和无进展生存期。采用累积发病率法估计转移灶控制率(MC)。采用Wilcoxon检验比较生存估计值。使用Cox比例风险模型评估MC和OS的预后因素,似然比也用于组间比较。
每个转移灶评估的PET扫描中位数为6次(范围2 - 6次)。SFED中位数为42.8 Gy(范围18 - 56.4 Gy),生物等效剂量中位数为254.4 Gy(范围100.8 - 540 Gy)。20%的患者接受化疗,59%的患者接受免疫治疗:粒细胞-巨噬细胞集落刺激因子(64%)和伊匹单抗(34%)。1年和3年时的MC分别为94%和90%。1年和3年时的OS分别为74%和27%。90%的患者在中位2.8个月(范围0.4 - 25.2个月)时达到完全缓解。SFED >24 Gy与MC改善相关(93%对75%,P = 0.01)。3级及以上急性和晚期毒性分别为4%和11%,无5级毒性。
颅外转移性MM的SBRT后PET/CT在中位2.8个月时导致高完全缓解率,SFED >24 Gy可实现持久的MC。对于MM患者,尤其是寡转移患者,除手术和消融外,应与患者讨论SBRT。