Hall Eric W, Morris Sapna B, Moore Brittany K, Erasmus Linda, Odendaal Ronel, Menzies Heather, van der Walt Martie, Smith Sarah E
From the *Department of Epidemiology, Emory University, Atlanta, Georgia; †U.S. Centers for Disease Control and Prevention, Atlanta, Georgia; ‡National Institute for Communicable Diseases, National Health Laboratory Service, Johannesburg, South Africa; and §South African Medical Research Council, Pretoria, South Africa.
Pediatr Infect Dis J. 2017 Dec;36(12):e322-e327. doi: 10.1097/INF.0000000000001691.
To describe outcomes of HIV-infected pediatric patients with drug-resistant tuberculosis (DR TB).
Demographic, clinical and laboratory data from charts of pediatric patients treated for DR TB during 2005-2008 were collected retrospectively from 5 multi-DR TB hospitals in South Africa. Data were summarized, and Pearson χ test or Fisher exact test was used to assess differences in variables of interest by HIV status. A time-to-event analysis was conducted using days from start of treatment to death. Variables of interest were first assessed using the Kaplan-Meier method. Cox proportional hazard models were fit to estimate crude and adjusted hazard ratios.
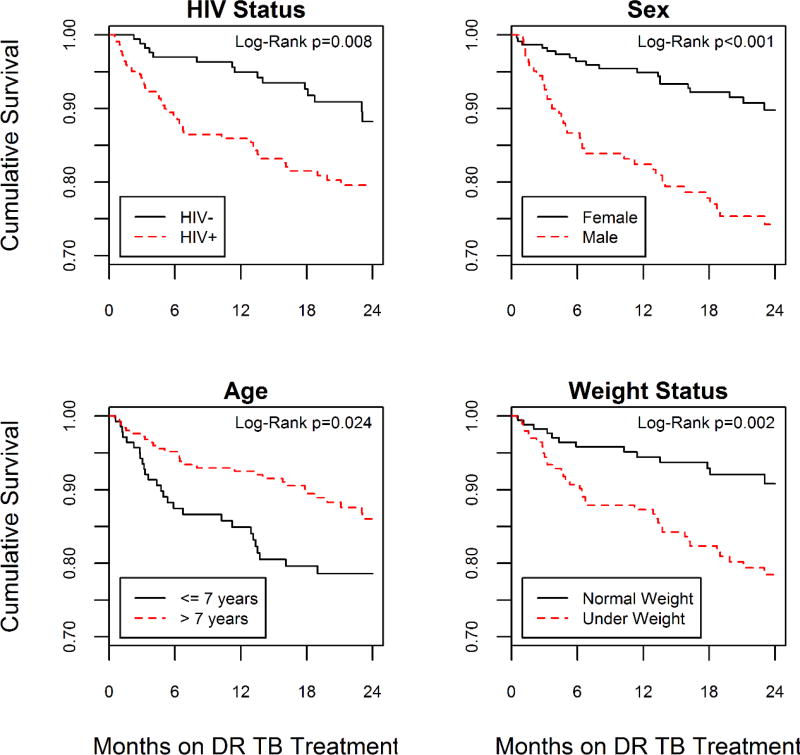
Of 423 eligible participants, 398 (95%) had culture-confirmed DR TB and 238 (56%) were HIV infected. A total of 54% were underweight, 42% were male and median age was 10.7 years (interquartile range: 5.5-15.3). Of the 423 participants, 245 (58%) were successfully treated, 69 (16%) died, treatment failed in 3 (1%), 36 (9%) were lost to follow-up and 70 (17%) were still on treatment, transferred or had unknown outcomes. Time to death differed by HIV status (P = 0.008), sex (P < 0.001), year of tuberculosis diagnosis (P = 0.05) and weight status (P = 0.002). Over the 2-year risk period, the adjusted rate of death was 2-fold higher among participants with HIV compared with HIV-negative participants (adjusted hazard ratio = 2.28; 95% confidence interval: 1.11-4.68).
Male, underweight and HIV-infected children with DR TB were more likely to experience death when compared with other children with DR TB within this study population.
描述感染人类免疫缺陷病毒(HIV)的耐药性肺结核(DR TB)儿科患者的治疗结果。
回顾性收集2005年至2008年期间在南非5家多耐药性肺结核医院接受DR TB治疗的儿科患者病历中的人口统计学、临床和实验室数据。对数据进行汇总,并使用Pearson χ检验或Fisher精确检验按HIV感染状况评估感兴趣变量的差异。采用从治疗开始到死亡的天数进行生存分析。首先使用Kaplan-Meier方法评估感兴趣的变量。拟合Cox比例风险模型以估计粗风险比和调整后的风险比。
在423名符合条件的参与者中,398名(95%)经培养确诊为DR TB,238名(56%)感染了HIV。共有54%体重不足,42%为男性,中位年龄为10.7岁(四分位间距:5.5 - 15.3)。在423名参与者中,245名(58%)成功治愈,69名(16%)死亡,3名(1%)治疗失败,36名(9%)失访,70名(17%)仍在接受治疗、转诊或结局不明。死亡时间因HIV感染状况(P = 0.008)、性别(P < 0.001)、结核病诊断年份(P = 0.05)和体重状况(P = 0.002)而异。在2年的风险期内,与HIV阴性参与者相比,HIV感染参与者的调整后死亡率高出2倍(调整后的风险比 = 2.28;95%置信区间:1.11 - 4.68)。
在本研究人群中,与其他DR TB儿童相比,患有DR TB的男性、体重不足和HIV感染儿童更有可能死亡。