Mornand Pierre, Verret Catherine, Minodier Philippe, Faye Albert, Thellier Marc, Imbert Patrick
Service de pédiatrie générale, Hôpital d'enfants A. Trousseau, 26 avenue du Dr Arnold Netter, 75571 Paris cedex 12, France.
Institut de Recherche Biomédicale des Armées. BP 73, Brétigny Sur Orge Cedex, France.
PLoS One. 2017 Jul 27;12(7):e0180758. doi: 10.1371/journal.pone.0180758. eCollection 2017.
Malaria is a leading cause of imported febrile illnesses in pediatric travelers, but few studies have addressed severe imported pediatric malaria. We aimed to determine the risk factors and the features of imported pediatric severe malaria.
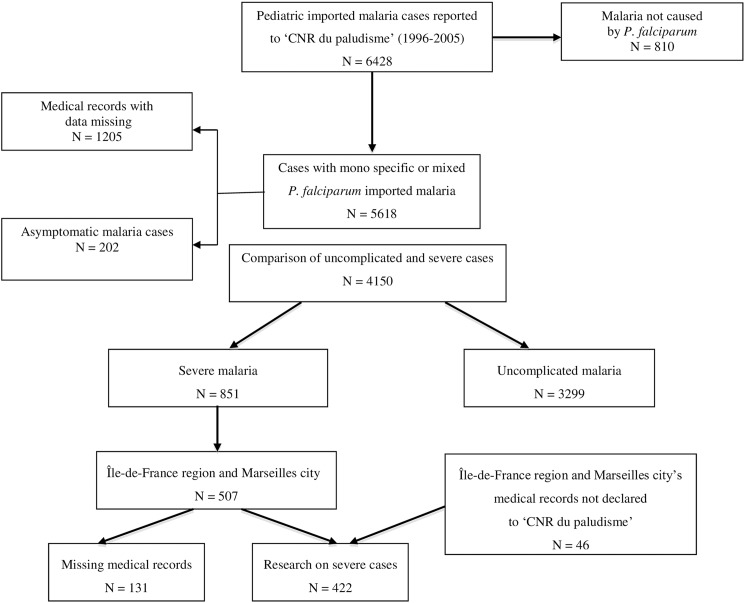
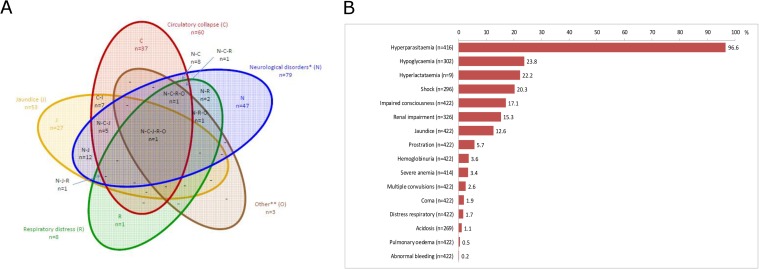
We conducted a retrospective, descriptive study using the French National Reference Center for Imported Malaria database, in children aged 0-15 years who were hospitalized with a falciparum malaria from January 1st 1996 to December 31th 2005. Uncomplicated and severe cases of falciparum malaria were compared to identify risk factors for severe cases. In the hospitals that reported more than five severe cases during the study period, we evaluated severe cases for prognostic factors and assessed the accuracy WHO criteria for predicting severity. Given the rarity of deaths, adverse outcomes were defined as requiring major therapeutic procedures (MTPs)-e.g., sedation, mechanical ventilation, nasal oxygen therapy, blood transfusions, hemodialysis, fluid resuscitation-or pediatric intensive care unit (PICU) admission.
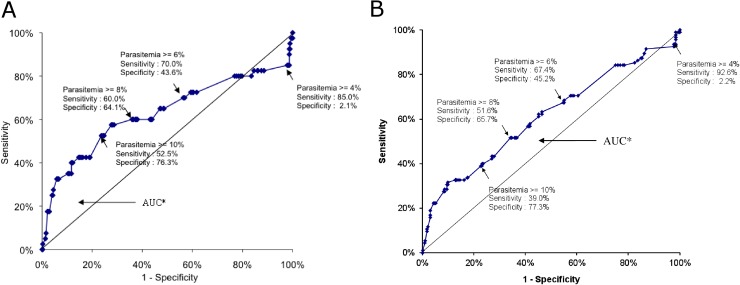
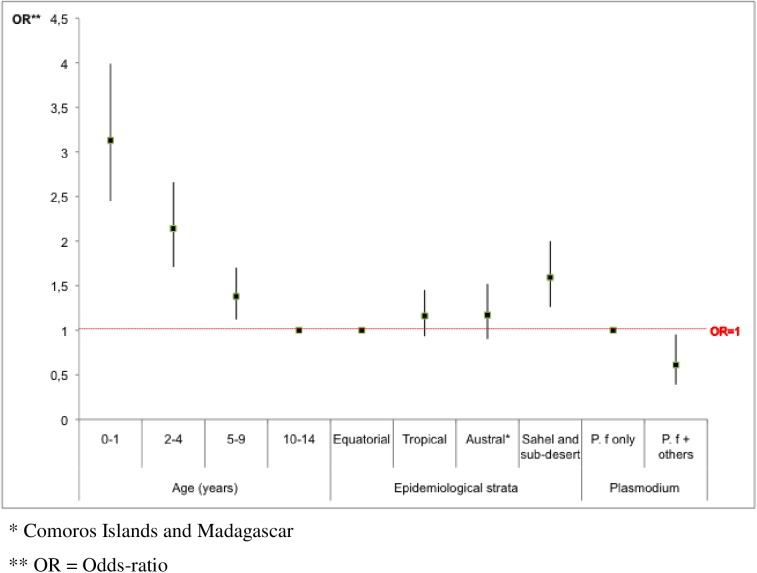
Of 4150 pediatric malaria cases included in the study, 3299 were uncomplicated and 851 (20.5%) were severe. Only one death was recorded during this period. Predictors for severe falciparum malaria were: age <2 years (OR = 3.2, 95% CI = 2.5-4.0, p <0.0001) and a travel in the Sahelian region (OR = 1.7, 95% CI = 1.3-2.0, p = 0.0001). Of 422 severe malaria cases, a stay in a Sahelian region, lack of chemoprophylaxis, age <2 years or thrombocytopenia <100 x 10^3/mm^3 predicted adverse outcomes. Except for the hyperparasitemia threshold of 4%, the main WHO 2000 criteria for severe malaria reliably predicted adverse outcomes. In our study, the threshold of parasitemia most predictive of a poor outcome was 8%.
In imported pediatric malaria, children younger than 2 years deserve particular attention. The main WHO 2000 criteria for severity are accurate, except for the threshold of hyperparasitemia, which should be revised.
疟疾是儿科旅行者输入性发热疾病的主要病因,但针对严重输入性儿科疟疾的研究较少。我们旨在确定输入性儿科严重疟疾的危险因素和特征。
我们利用法国国家输入性疟疾参考中心数据库,对1996年1月1日至2005年12月31日期间因恶性疟住院的0至15岁儿童进行了一项回顾性描述性研究。比较非复杂性和严重性恶性疟病例,以确定严重病例的危险因素。在研究期间报告了五例以上严重病例的医院,我们评估了严重病例的预后因素,并评估了世界卫生组织(WHO)预测严重性标准的准确性。鉴于死亡病例罕见,不良结局定义为需要进行重大治疗程序(MTP),如镇静、机械通气、鼻导管给氧治疗、输血、血液透析、液体复苏,或入住儿科重症监护病房(PICU)。
在纳入研究的4150例儿科疟疾病例中,3299例为非复杂性病例,851例(20.5%)为严重病例。在此期间仅记录到1例死亡。严重恶性疟的预测因素为:年龄<2岁(比值比[OR]=3.2,95%置信区间[CI]=2.5-至4.0,p<0.0001)和在萨赫勒地区旅行(OR=1.7,95%CI=1.3-2.0,p=0.0001)。在422例严重疟疾病例中,在萨赫勒地区停留、未进行化学预防、年龄<2岁或血小板减少<100×10³/mm³可预测不良结局。除高疟原虫血症阈值为4%外,WHO 2000年严重疟疾的主要标准可可靠地预测不良结局。在我们的研究中,最能预测不良结局的疟原虫血症阈值为8%。
在输入性儿科疟疾中,2岁以下儿童值得特别关注。WHO 2000年严重程度的主要标准是准确的,但高疟原虫血症阈值应予以修订。