Rose Sally B, Garrett Susan M, Stanley James, Pullon Susan R H
Department of Primary Health Care and General Practice, University of Otago, Wellington, PO Box 7343, Wellington South, 6242, New Zealand.
Biostatistical Group, University of Otago, Wellington, P O Box 7343, Wellington South, 6242, New Zealand.
BMC Infect Dis. 2017 Jul 28;17(1):526. doi: 10.1186/s12879-017-2635-y.
Testing for reinfection at 3 to 6 months following treatment for Chlamydia Trachomatis or Neisseria gonorrhoea is recommended in best practice sexual health management guidelines. This study aimed to describe rates of retesting and repeat positivity following diagnosis of chlamydia or gonorrhoea in a defined geographic region of New Zealand.
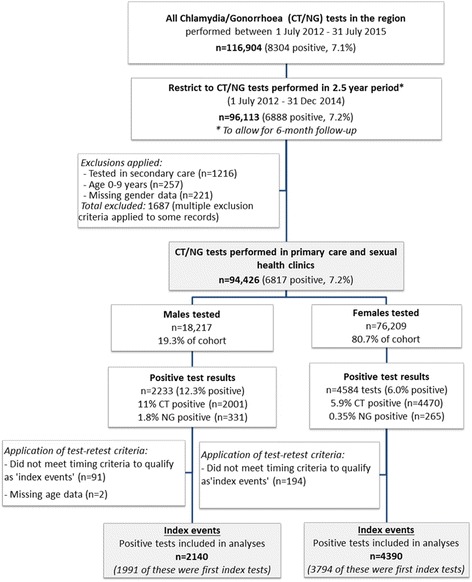
Retrospective cohort study in Wellington, New Zealand involving analysis of laboratory data for chlamydia and gonorrhoea tests performed in primary care and sexual health clinics (July 2012-July 2015).
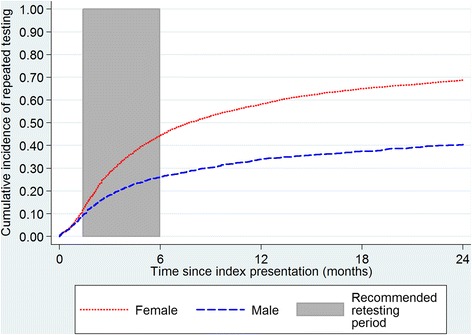
rate of retesting and rate of repeat positivity 6 weeks to 6 months after a positive result (index event). Kaplan-Meier curves were used to plot time from first index event to retest. Logistic regression modelling was used to determine the odds of retesting and repeat positivity between 6 weeks and 6 months of follow-up, adjusting for potential confounders (age, gender, ethnicity and socioeconomic deprivation).
Overall 29.4% (1919/6530) of the cohort was retested between 6 weeks and 6 months, with 18% (347/1919) of those retested returning positive results. Lower odds of retesting were observed for males (OR 0.4, 95% CI 0.34-0.48), and individuals of NZ Maori (OR 0.72, 0.61-0.85) and Pacific ethnicities (OR 0.49, 0.39-0.62, reference European). Factors associated with higher odds of repeat positivity on retesting included male gender (OR 2.0, 1.14-2.82), age 15-19 years (OR 1.78, 1.32-2.41, reference 20-24 years), chlamydia/gonorrhoea co-infection (OR 2.39, 1.32-4.35, reference chlamydia only), Maori (OR 1.6, 1.18-2.17) and Pacific ethnicities (OR 1.88, 1.22-2.9, reference European).
We observed low adherence to STI retesting guidelines, and marked gender and ethnic disparities in rates of retesting and repeat positivity. Low retesting rates are suggestive of low levels of awareness of this aspect of patient management, and an absence of a systematic approach to retesting. High rates of repeat positivity reinforce the importance of advising patients about reducing their risk of reinfection, including notification and treatment of all recent sexual partners. Greater priority needs to be placed on increasing retesting and reducing rates of reinfection, with strategies implemented to improve these important aspects of patient care and population STI control.
最佳实践性健康管理指南建议,在沙眼衣原体或淋病奈瑟菌治疗后3至6个月进行再感染检测。本研究旨在描述新西兰一个特定地理区域内衣原体或淋病诊断后的重新检测率和再次阳性率。
在新西兰惠灵顿进行的回顾性队列研究,涉及分析在初级保健和性健康诊所进行的衣原体和淋病检测的实验室数据(2012年7月至2015年7月)。
阳性结果(索引事件)后6周至6个月的重新检测率和再次阳性率。使用Kaplan-Meier曲线绘制从首次索引事件到重新检测的时间。使用逻辑回归模型确定随访6周和6个月之间重新检测和再次阳性的几率,并对潜在混杂因素(年龄、性别、种族和社会经济剥夺)进行调整。
总体而言,队列中有29.4%(1919/6530)在6周和6个月之间进行了重新检测,其中18%(347/1919)的重新检测者返回了阳性结果。男性(OR 0.4,95% CI 0.34 - 0.48)、新西兰毛利人(OR 0.72,0.61 - 0.85)和太平洋族裔(OR 0.49,0.39 - 0.62,参照欧洲裔)的重新检测几率较低。重新检测时与再次阳性几率较高相关的因素包括男性(OR 2.0,1.14 - 2.82)、15 - 19岁年龄组(OR 1.78,1.32 - 2.41,参照20 - 24岁年龄组)、衣原体/淋病合并感染(OR 2.39,1.32 - 4.35,参照仅衣原体感染)、毛利人(OR 1.6,1.18 - 2.17)和太平洋族裔(OR 1.88,1.22 - 2.9,参照欧洲裔)。
我们观察到对性传播感染重新检测指南的依从性较低,并且在重新检测率和再次阳性率方面存在明显的性别和种族差异。低重新检测率表明对患者管理这一方面的认识水平较低,并且缺乏系统的重新检测方法。高再次阳性率强化了向患者提供关于降低再感染风险建议的重要性,包括通知和治疗所有近期性伴侣。需要更加优先地提高重新检测率并降低再感染率,实施策略以改善患者护理和人群性传播感染控制的这些重要方面。