Kray Jared E, Dombrovskiy Viktor Y, Vogel Todd R
Department of Surgery, Division of Vascular Surgery, School of Medicine, University of Missouri, Columbia, MO.
Department of Surgery, Rutgers-Robert Wood Johnson Medical School, New Brunswick, NJ, USA.
Vasc Health Risk Manag. 2017 Jul 14;13:269-274. doi: 10.2147/VHRM.S137698. eCollection 2017.
Angiotensin-converting enzyme inhibitors (ACEIs) have not been well evaluated in conjunction with lower extremity revascularization (LER). This study evaluated freedom from amputation in patients who underwent either an open (OPEN) or endovascular (ENDO) revascularization with and without utilization of an ACEI.
Patients who underwent LER were identified from 2007-2008 Medicare Provider Analysis and Review files. Demographics, comorbidities, and disease severity were obtained. Post-procedural use of an ACEI was confirmed using combining them with National Drug Codes and Part D Files. Outcomes were analyzed using chi-square analysis, Kaplan-Meier test, and Cox regression.
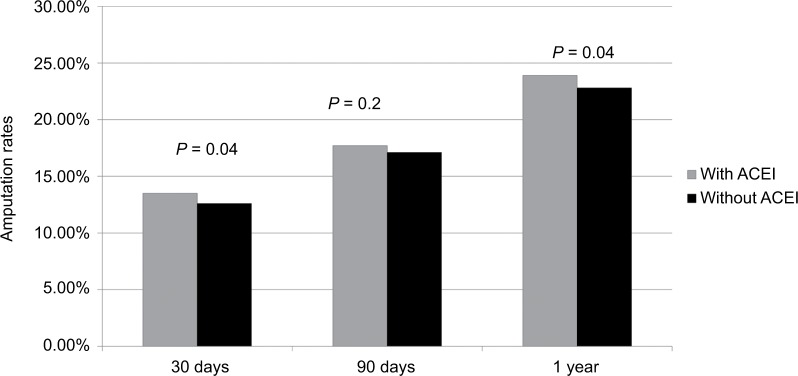
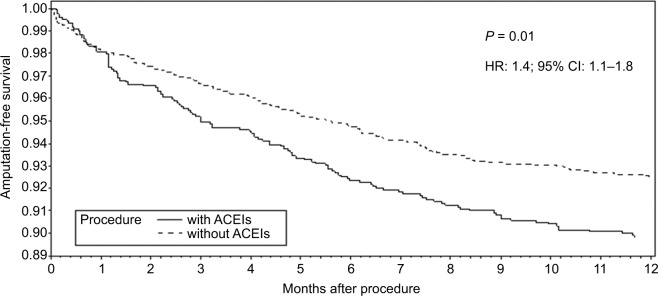
We identified 22,954 patients who underwent LER: 8,128 (35.4%) patients with claudication, 3,056 (13.3%) with rest pain, and 11,770 (51.3%) with ulceration or gangrene. More patients underwent ENDO (14,353) than OPEN (8,601) revascularization and 38% of the cohort was taking an ACEI. Overall, ACEI utilization compared to patients not taking ACEI was not associated with lower amputation rates at 30 days (13.5% vs. 12.6%), 90 days (17.7% vs. 17.1%), or 1 year (23.9% vs. 22.8%) (>0.05 for all). After adjustment for comorbidities, ACEI utilization was associated with higher amputation rates for patients with rest pain (hazard ratio: 1.4; 95% confidence interval: 1.1-1.8).
ACEI utilization was not associated with overall improved rates of amputation-free survival or overall survival in the vascular surgery population. However, an important finding of this study was that patients presenting with a diagnosis of rest pain and taking an ACEI who underwent a LER had statistically higher amputation rates and a lower amputation-free survival at 1 year. Further analysis is needed to delineate best medical management for patients with critical limb ischemia and taking ACEI who undergo vascular revascularization.
血管紧张素转换酶抑制剂(ACEI)与下肢血管重建术(LER)联合使用的效果尚未得到充分评估。本研究评估了接受开放性(OPEN)或血管腔内(ENDO)血管重建术且使用或未使用ACEI的患者的截肢-free情况。
从2007 - 2008年医疗保险提供者分析与审查文件中识别出接受LER的患者。获取人口统计学、合并症和疾病严重程度信息。通过将其与国家药品代码和D部分文件相结合来确认术后ACEI的使用情况。使用卡方分析、Kaplan-Meier检验和Cox回归分析结果。
我们识别出22,954例接受LER的患者:8,128例(35.4%)间歇性跛行患者,3,056例(13.3%)静息痛患者,11,770例(51.3%)溃疡或坏疽患者。接受ENDO血管重建术的患者(14,353例)多于OPEN血管重建术的患者(8,601例),且队列中有38%的患者正在服用ACEI。总体而言,与未服用ACEI的患者相比,ACEI的使用在30天(13.5%对12.6%)、90天(17.7%对17.1%)或1年(23.9%对22.8%)时与较低的截肢率无关(所有P>0.05)。在对合并症进行调整后,ACEI的使用与静息痛患者的较高截肢率相关(风险比:1.4;95%置信区间:1.1 - 1.8)。
在血管外科人群中,ACEI的使用与无截肢生存率或总生存率的总体改善无关。然而,本研究的一个重要发现是,诊断为静息痛且服用ACEI并接受LER的患者在1年时截肢率在统计学上更高,无截肢生存率更低。需要进一步分析以确定对患有严重肢体缺血且服用ACEI并接受血管重建术的患者的最佳药物治疗方案。