Brault Marie A, Ngure Kenneth, Haley Connie A, Kabaka Stewart, Sergon Kibet, Desta Teshome, Mwinga Kasonde, Vermund Sten H, Kipp Aaron M
University of Connecticut, Department of Anthropology, Storrs, Connecticut, United States of America.
Jomo Kenyatta University of Agriculture and Technology, School of Public Health, Nairobi, Kenya.
PLoS One. 2017 Aug 1;12(8):e0181777. doi: 10.1371/journal.pone.0181777. eCollection 2017.
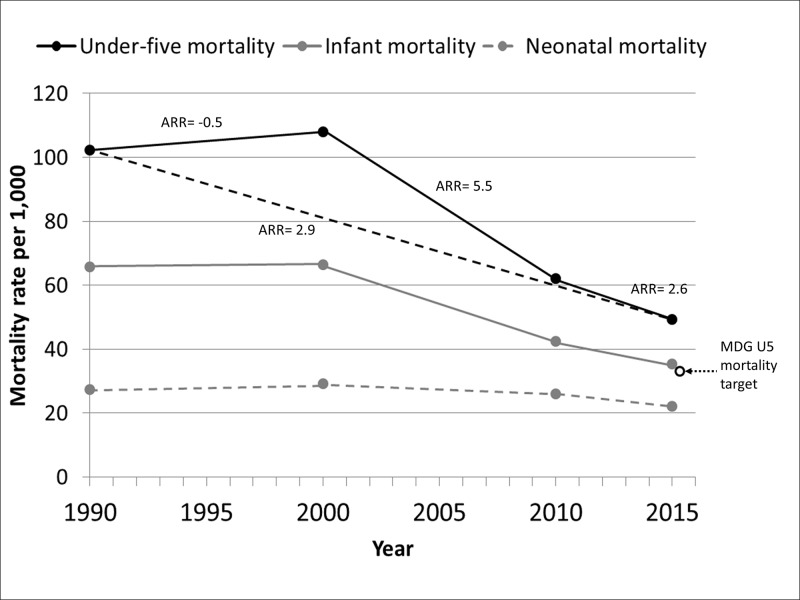
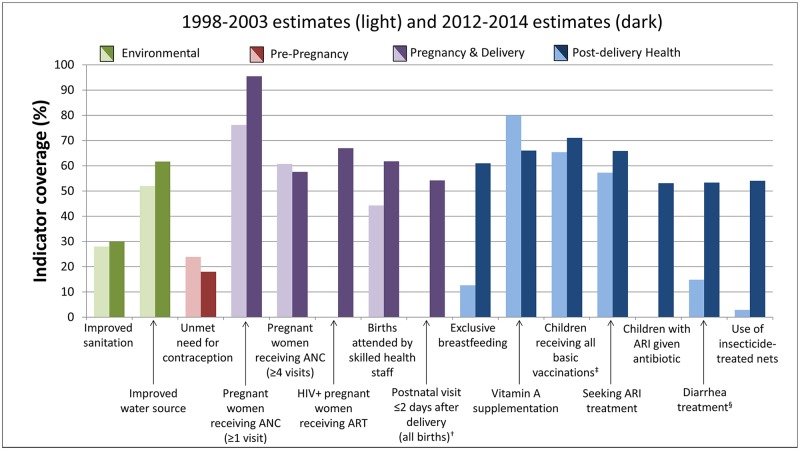
As of 2015, only 12 countries in the World Health Organization's AFRO region had met Millennium Development Goal #4 (MDG#4) to reduce under-five mortality by two-thirds by 2015. Given the variability across the African region, a four-country study was undertaken to examine barriers and facilitators of child survival prior to 2015. Kenya was one of the countries selected for an in-depth case study due to its insufficient progress in reducing under-five mortality, with only a 28% reduction between 1990 and 2013. This paper presents indicators, national documents, and qualitative data describing the factors that have both facilitated and hindered Kenya's efforts in reducing child mortality. Key barriers identified in the data were widespread socioeconomic and geographic inequities in access and utilization of maternal, neonatal, and child health (MNCH) care. To reduce these inequities, Kenya implemented three major policies/strategies during the study period: removal of user fees, the Kenya Essential Package for Health, and the Community Health Strategy. This paper uses qualitative data and a policy review to explore the early impacts of these efforts. The removal of user fees has been unevenly implemented as patients still face hidden expenses. The Kenya Essential Package for Health has enabled construction and/or expansion of healthcare facilities in many areas, but facilities struggle to provide Emergency Obstetric and Neonatal Care (EmONC), neonatal care, and many essential medicines and commodities. The Community Health Strategy appears to have had the most impact, improving referrals from the community and provision of immunizations, malaria prevention, and Prevention of Mother-to-Child Transmission of HIV. However, the Community Health Strategy is limited by resources and thus also unevenly implemented in many areas. Although insufficient progress was made pre-2015, with additional resources and further scale-up of new policies and strategies Kenya can make further progress in child survival.
截至2015年,世界卫生组织非洲区域办事处(AFRO)所辖区域内仅有12个国家实现了千年发展目标4(MDG#4),即在2015年之前将五岁以下儿童死亡率降低三分之二。鉴于非洲区域情况各异,开展了一项四国研究,以考察2015年之前儿童生存的障碍和促进因素。肯尼亚是被选中进行深入案例研究的国家之一,因其在降低五岁以下儿童死亡率方面进展不足,1990年至2013年间仅降低了28%。本文介绍了相关指标、国家文件以及定性数据,描述了促进和阻碍肯尼亚降低儿童死亡率努力的因素。数据中确定的主要障碍是在孕产妇、新生儿和儿童健康(MNCH)护理的获取和利用方面广泛存在的社会经济和地理不平等。为减少这些不平等,肯尼亚在研究期间实施了三项主要政策/战略:取消用户收费、《肯尼亚基本卫生服务包》和《社区卫生战略》。本文使用定性数据和政策审查来探讨这些努力的早期影响。取消用户收费的实施情况参差不齐,因为患者仍然面临隐性费用。《肯尼亚基本卫生服务包》使许多地区的医疗设施得以建设和/或扩建,但这些设施难以提供急诊产科和新生儿护理(EmONC)、新生儿护理以及许多基本药品和用品。《社区卫生战略》似乎产生了最大影响,改善了社区转诊以及免疫接种、疟疾预防和预防母婴传播艾滋病毒的服务提供。然而,《社区卫生战略》受到资源限制,因此在许多地区的实施也不均衡。尽管2015年之前进展不足,但通过增加资源以及进一步扩大新政策和战略的规模,肯尼亚在儿童生存方面可以取得更大进展。