Landsman-Blumberg Pamela B, Katz Nathaniel, Gajria Kavita, D'Souza Anna O, Chaudhari Sham L, Yeung Paul P, White Richard
Real-World Evidence, Xcenda LLC, Palm Harbor, FL.
Analgesic Solutions, Natick, MA.
J Pain Res. 2017 Jul 21;10:1713-1722. doi: 10.2147/JPR.S130913. eCollection 2017.
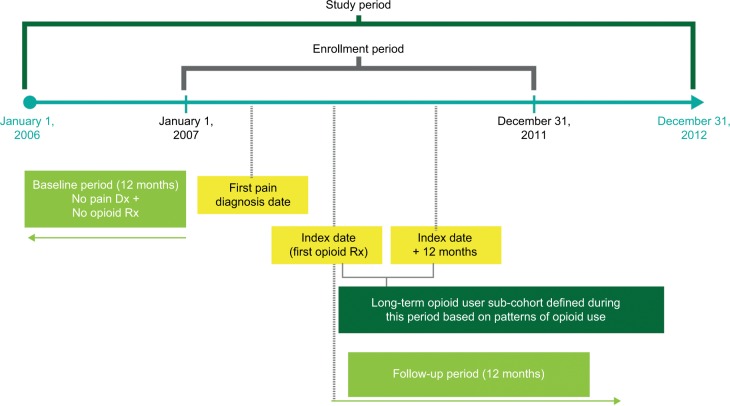
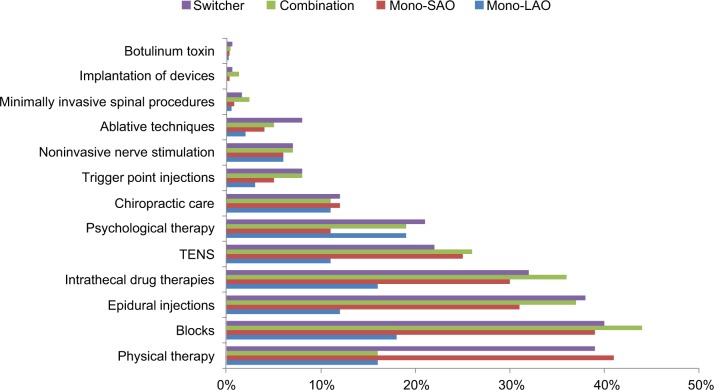
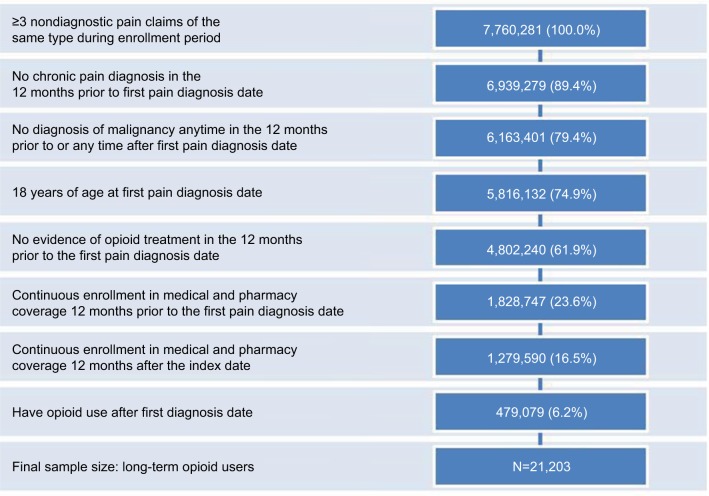
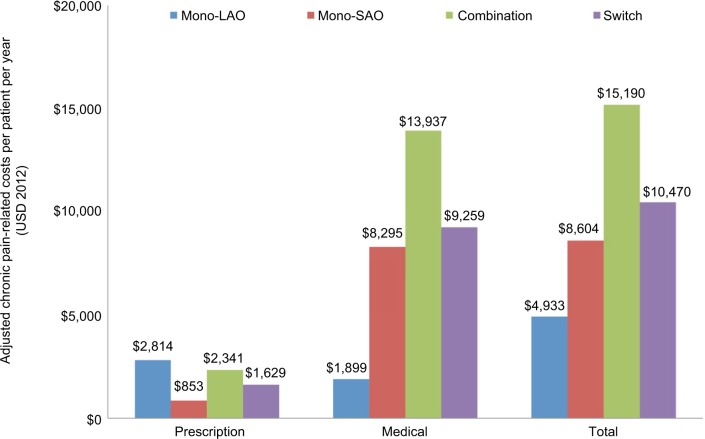
The study assessed 12-month chronic pain (CP)-related health care utilization and costs among chronic noncancer pain (CNCP) patients who initiated various long-term opioid treatments. Treatments included monotherapy with long-acting opioids (mono-LAOs), mono-therapy with short-acting opioids (mono-SAOs), both LAOs and SAOs (combination), and opioid therapy initiated with SAO or LAO and switched to the other class (switch). Using MarketScan claims databases (2006-2012), we identified CNCP patients with ≥90 days opioid supply after pain diagnosis and continuous enrollment 12 months before pain diagnosis (baseline period) and 12 months after opioid start (post-index period). Outcomes included CP-related health care utilization and costs. Among CNCP patients (n=21,203), the cohort distribution was 74% mono-SAOs, 22% combination, 2% mono-LAOs, and 2% switch. During follow-up, the average daily morphine equivalent dose was highest in mono-LAO patients (96.4 mg) compared with combination patients (89.8 mg), switch patients (64.3 mg), and mono-SAO patients (36.2 mg). After adjusting for baseline differences, the mono-LAO cohort had lower total CP-related costs ($4,933) compared with the mono-SAO ($8,604), switch ($10,470), and combination ($15,190) cohorts (all: <0.05). Mono-LAO patients had greater CP-related prescription costs but lower medical costs than the other cohorts during the follow-up period, including lower CP-related hospitalizations (1% vs 11%-20%), emergency department visits (4% vs 11%-18%), and diagnostic radiology use (21% vs 54%-61%) (all: <0.001). Use of pain-related medications and other treatment modalities was also significantly lower in the mono-LAO cohort relative to the other cohorts. CNCP patients using long-term monotherapy with LAOs had the lowest CP-related total health care costs in the 12 months after opioid initiation compared with mono-SAO, switch, or combination patients despite higher opioid daily doses and higher prescription costs. Future research accounting for severity and duration of pain would aid in determining the optimal long-term opioid regimen for CNCP patients.
该研究评估了开始接受各种长期阿片类药物治疗的慢性非癌性疼痛(CNCP)患者中与12个月慢性疼痛(CP)相关的医疗保健利用情况和费用。治疗方法包括长效阿片类药物单药治疗(单药-LAO)、短效阿片类药物单药治疗(单药-SAO)、LAO和SAO联合使用(联合治疗),以及开始使用SAO或LAO并转换为另一类药物的阿片类药物治疗(转换治疗)。利用MarketScan理赔数据库(2006 - 2012年),我们确定了疼痛诊断后阿片类药物供应≥90天且在疼痛诊断前12个月(基线期)和阿片类药物开始使用后12个月(索引后期)持续参保的CNCP患者。结局指标包括与CP相关的医疗保健利用情况和费用。在CNCP患者(n = 21,203)中,队列分布为74%单药-SAO、22%联合治疗、2%单药-LAO和2%转换治疗。在随访期间,单药-LAO患者的平均每日吗啡当量剂量最高(96.4毫克),相比之下,联合治疗患者为(89.8毫克)、转换治疗患者为(64.3毫克)、单药-SAO患者为(36.2毫克)。在对基线差异进行调整后,与单药-SAO(8604美元)、转换治疗(10470美元)和联合治疗(15190美元)队列相比,单药-LAO队列的CP相关总费用较低(4933美元)(所有比较:P < 0.05)。在随访期间,单药-LAO患者的CP相关处方费用较高,但医疗费用低于其他队列,包括CP相关住院率较低(1%对11% - 20%)、急诊科就诊率较低(4%对11% - 18%)以及诊断性放射检查使用率较低(21%对54% - 61%)(所有比较:P < 0.001)。相对于其他队列,单药-LAO队列中与疼痛相关药物和其他治疗方式的使用也显著较低。与单药-SAO、转换治疗或联合治疗患者相比,使用LAO进行长期单药治疗的CNCP患者在阿片类药物开始使用后的12个月内CP相关的总医疗保健费用最低,尽管其每日阿片类药物剂量较高且处方费用较高。考虑疼痛严重程度和持续时间的未来研究将有助于确定CNCP患者的最佳长期阿片类药物治疗方案。