Takayama Atsushi, Nagamine Takahiko, Matsumoto Yoshinobu, Nakamura Masaru
Department of Family Medicine, Iwakuni Municipal Miwa Hospital, Japan.
Jichi Medical University Center for Community Medicine, Division of Community and Family Medicine, Japan.
Intern Med. 2019 Jun 15;58(12):1791-1794. doi: 10.2169/internalmedicine.2059-18. Epub 2019 Feb 25.
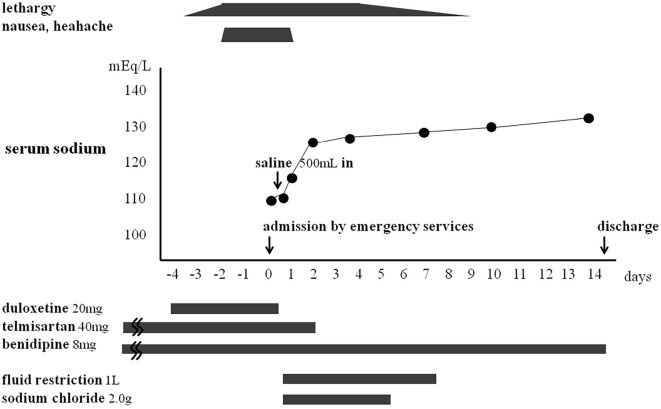
We encountered a case of syndrome of inappropriate antidiuretic hormone secretion (SIADH) caused by duloxetine, serotonin and norepinephrine reuptake inhibitor (SNRI). A 74-year-old woman complaining of severe lethargy was transferred to our emergency department. Her serum sodium level was 109 mEq/L. Plasma hypo-osmolality with urine normo-osmolality was observed, indicating SIADH. Her essential hypertension had long been treated with telmisartan, and she had just started duloxetine 20 mg/day for chronic musculoskeletal pain 4 days prior to admission. On prescribing duloxetine in the primary care setting, clinicians should be aware of the possibility of duloxetine-induced hyponatremia, particularly in combination with telmisartan.
我们遇到了一例由度洛西汀(一种5-羟色胺和去甲肾上腺素再摄取抑制剂,SNRI)引起的抗利尿激素分泌异常综合征(SIADH)。一名74岁女性因严重嗜睡被转诊至我院急诊科。她的血清钠水平为109 mEq/L。观察到血浆低渗而尿液等渗,提示为SIADH。她的原发性高血压长期使用替米沙坦治疗,入院前4天因慢性肌肉骨骼疼痛刚开始服用度洛西汀,剂量为20 mg/天。在基层医疗环境中开具度洛西汀处方时,临床医生应意识到度洛西汀诱发低钠血症的可能性,尤其是与替米沙坦合用时。