Hesam-Shariati Negin, Trinh Terry, Thompson-Butel Angelica G, Shiner Christine T, McNulty Penelope A
Neuroscience Research Australia, Sydney, NSW, Australia.
School of Medical Science, University of New South Wales, Sydney, NSW, Australia.
Front Neurol. 2017 Jul 20;8:277. doi: 10.3389/fneur.2017.00277. eCollection 2017.
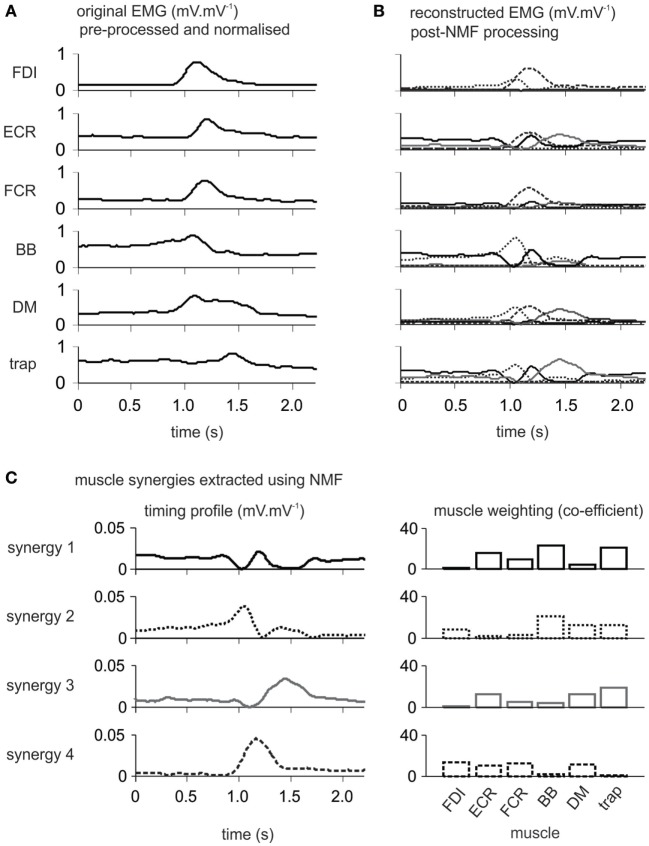
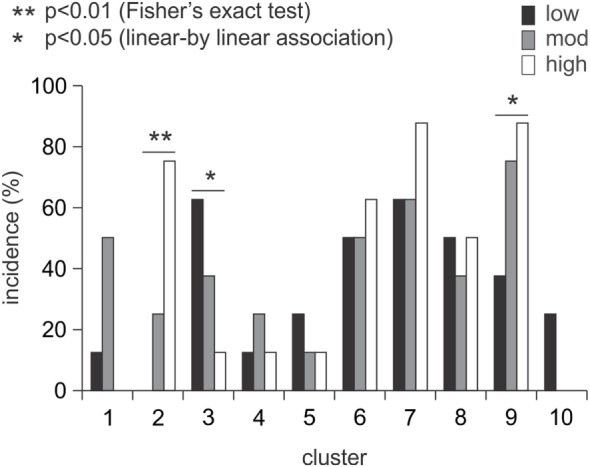
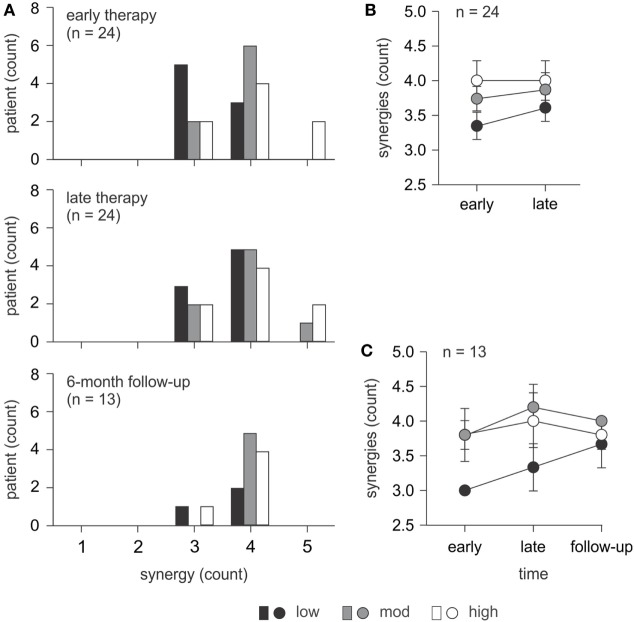
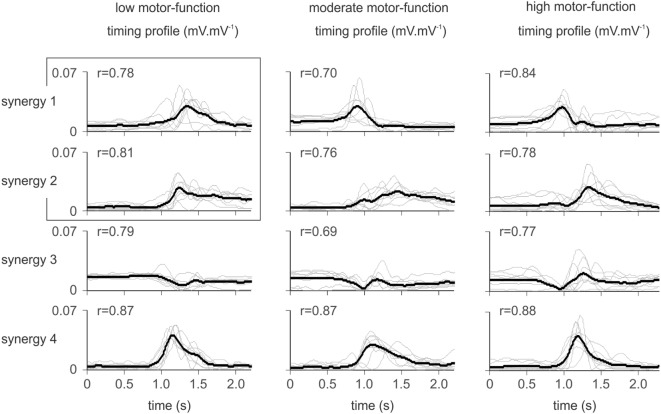
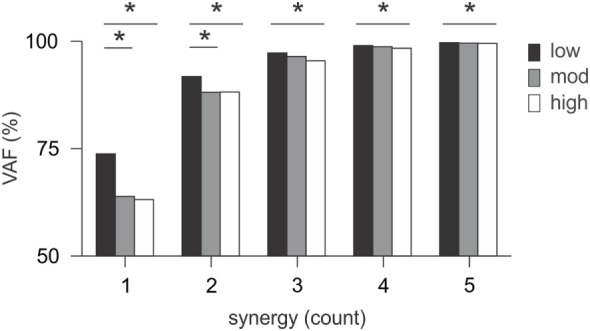
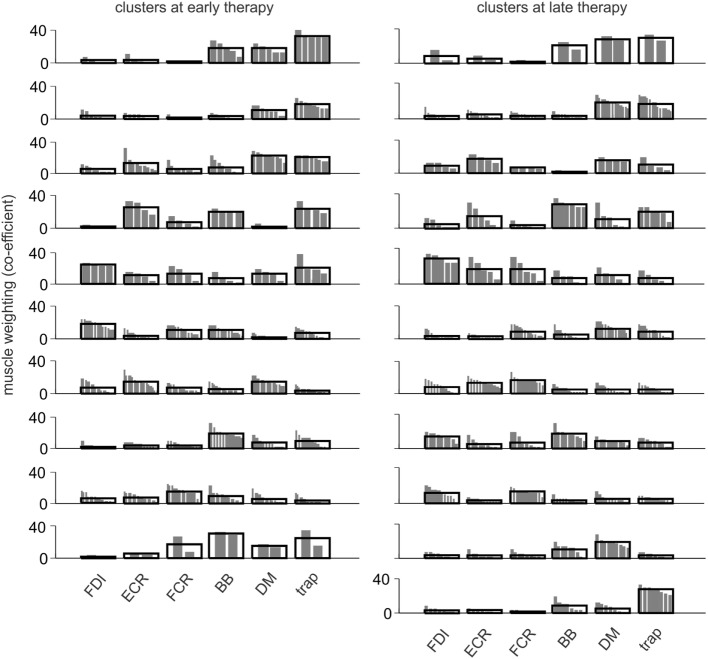
Fine motor control is achieved through the coordinated activation of groups of muscles, or "muscle synergies." Muscle synergies change after stroke as a consequence of the motor deficit. We investigated the pattern and longitudinal changes in upper limb muscle synergies therapy in a largely unconstrained movement in patients with a broad spectrum of poststroke residual voluntary motor capacity. Electromyography (EMG) was recorded using wireless telemetry from 6 muscles acting on the more-affected upper body in 24 stroke patients at early and late therapy during formal Wii-based Movement Therapy (WMT) sessions, and in a subset of 13 patients at 6-month follow-up. Patients were classified with low, moderate, or high motor-function. The Wii-baseball swing was analyzed using a non-negative matrix factorization (NMF) algorithm to extract muscle synergies from EMG recordings based on the temporal activation of each synergy and the contribution of each muscle to a synergy. Motor-function was clinically assessed immediately pre- and post-therapy and at 6-month follow-up using the Wolf Motor Function Test, upper limb motor Fugl-Meyer Assessment, and Motor Activity Log Quality of Movement scale. Clinical assessments and game performance demonstrated improved motor-function for all patients at post-therapy ( < 0.01), and these improvements were sustained at 6-month follow-up ( > 0.05). NMF analysis revealed fewer muscle synergies (mean ± SE) for patients with low motor-function (3.38 ± 0.2) than those with high motor-function (4.00 ± 0.3) at early therapy ( = 0.036) with an association trend between the number of synergies and the level of motor-function. By late therapy, there was no significant change between groups, although there was a pattern of increase for those with low motor-function over time. The demonstrated differences with motor-function level ( < 0.05) but not time. Cluster analysis of the pooled synergies highlighted the therapy-induced change in muscle activation. Muscle synergies could be identified for all patients during therapy activities. These results show less complexity and more co-activation in the muscle activation for patients with low motor-function as a higher number of muscle synergies reflects greater movement complexity and task-related phasic muscle activation. The increased number of synergies and changes within synergies by late-therapy suggests improved motor control and movement quality with more distinct phases of movement.
精细运动控制是通过肌肉群的协同激活来实现的,即“肌肉协同作用”。中风后,由于运动功能缺陷,肌肉协同作用会发生变化。我们研究了上肢肌肉协同作用的模式及其纵向变化,这些患者在接受治疗时大多进行无限制运动,涵盖了广泛的中风后残余自主运动能力范围。在基于Wii的正式运动疗法(WMT)疗程的早期和晚期,使用无线遥测技术记录了24名中风患者受影响更严重的上半身6块肌肉的肌电图(EMG),并且在6个月随访时对13名患者的子集进行了记录。患者被分为低、中、高运动功能组。使用非负矩阵分解(NMF)算法分析Wii棒球挥杆动作,以便根据每个协同作用的时间激活以及每块肌肉对协同作用的贡献,从EMG记录中提取肌肉协同作用。在治疗前、治疗后以及6个月随访时,使用Wolf运动功能测试、上肢运动Fugl-Meyer评估和运动活动日志运动质量量表对运动功能进行临床评估。临床评估和游戏表现表明,所有患者在治疗后运动功能均有改善(<0.01),并且这些改善在6个月随访时得以维持(>0.05)。NMF分析显示,在早期治疗时,低运动功能患者(3.38±0.2)的肌肉协同作用比高运动功能患者(4.00±0.3)更少(=0.036),协同作用数量与运动功能水平之间存在关联趋势。到晚期治疗时,两组之间没有显著变化,尽管低运动功能患者的协同作用数量随时间有增加的趋势。结果表明与运动功能水平存在差异(<0.05),但与时间无关。对合并协同作用的聚类分析突出了治疗引起的肌肉激活变化。在治疗活动期间,可以为所有患者识别出肌肉协同作用。这些结果表明,低运动功能患者的肌肉激活复杂性较低且共同激活更多,因为更多的肌肉协同作用反映了更大的运动复杂性和与任务相关的阶段性肌肉激活。晚期治疗时协同作用数量的增加以及协同作用内部的变化表明,运动控制和运动质量得到改善,运动阶段更加明显。