Zhao Kunkun, Zhang Zhisheng, Wen Haiying, Liu Bin, Li Jianqing, Scano Alessandro
School of Biomedical Engineering and Informatics, Nanjing Medical University, Nanjing, China.
School of Mechanical Engineering, Southeast University, Nanjing, China.
Heliyon. 2023 May 11;9(5):e16202. doi: 10.1016/j.heliyon.2023.e16202. eCollection 2023 May.
Muscle synergies have been proposed as a strategy employed by the central nervous system to control movements. Muscle synergy analysis is a well-established framework to examine the pathophysiological basis of neurological diseases and has been applied for analysis and assessment in clinical applications in the last decades, even if it has not yet been widely used in clinical diagnosis, rehabilitative treatment and interventions. Even if inconsistencies in the outputs among studies and lack of a normative pipeline including signal processing and synergy analysis limit the progress, common findings and results are identifiable as a basis for future research. Therefore, a literature review that summarizes methods and main findings of previous works on upper limb muscle synergies in clinical environment is needed to i) summarize the main findings so far, ii) highlight the barriers limiting their use in clinical applications, and iii) suggest future research directions needed for facilitating translation of experimental research to clinical scenarios.
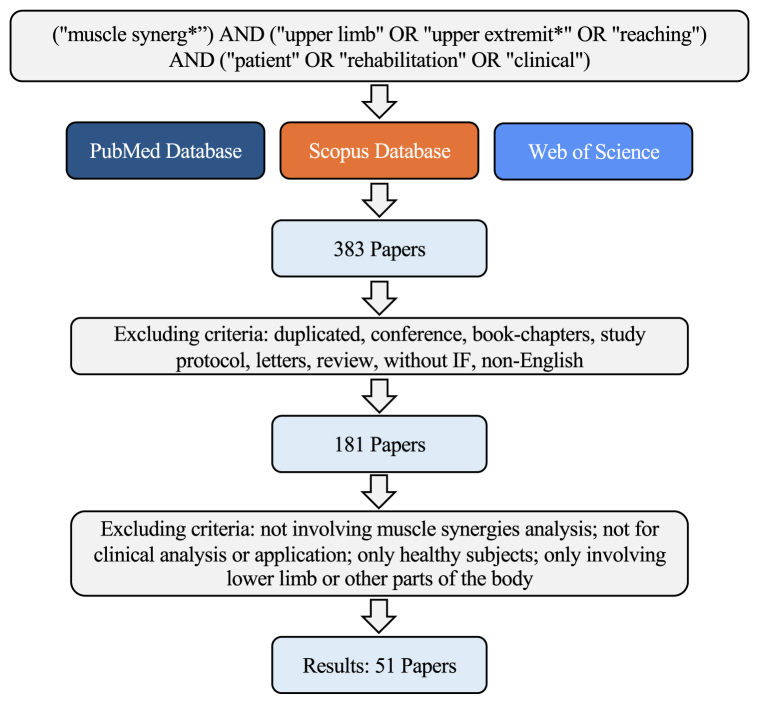
Articles in which muscle synergies were used to analyze and assess upper limb function in neurological impairments were reviewed. The literature research was conducted in Scopus, PubMed, and Web of Science. Experimental protocols (e.g., the aim of the study, number and type of participants, number and type of muscles, and tasks), methods (e.g., muscle synergy models and synergy extraction methods, signal processing methods), and the main findings of eligible studies were reported and discussed.
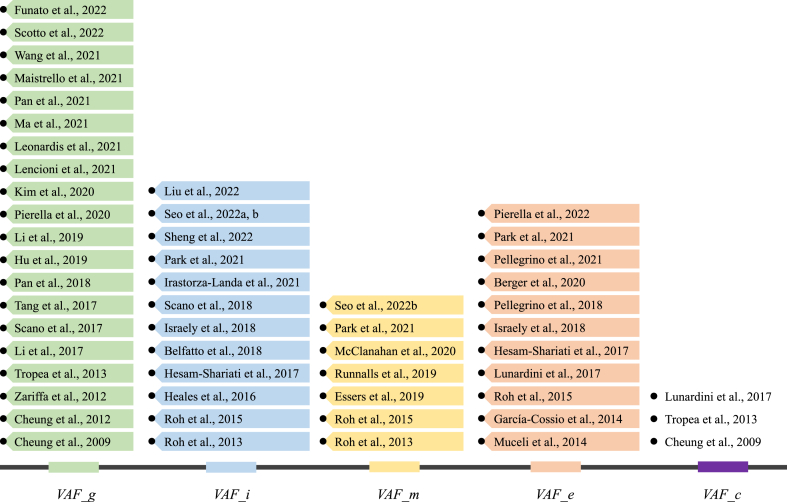
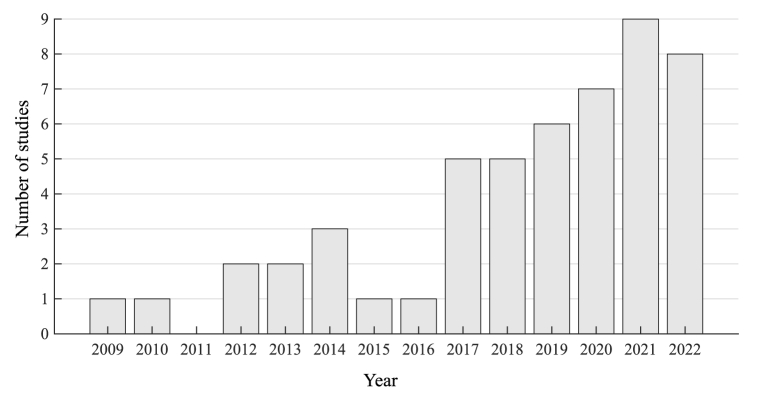
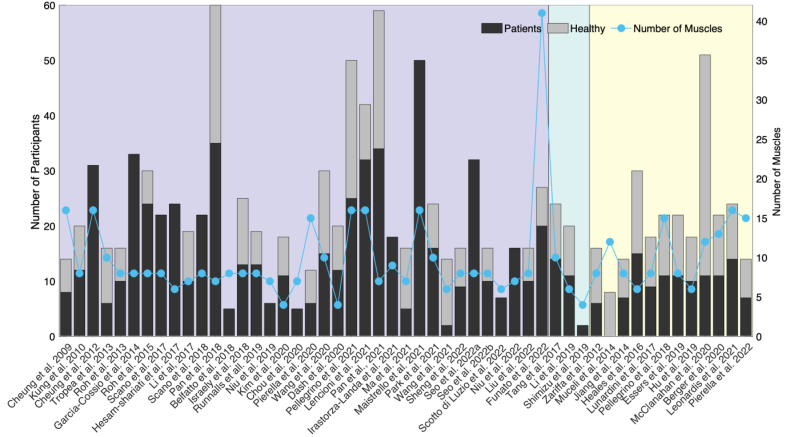
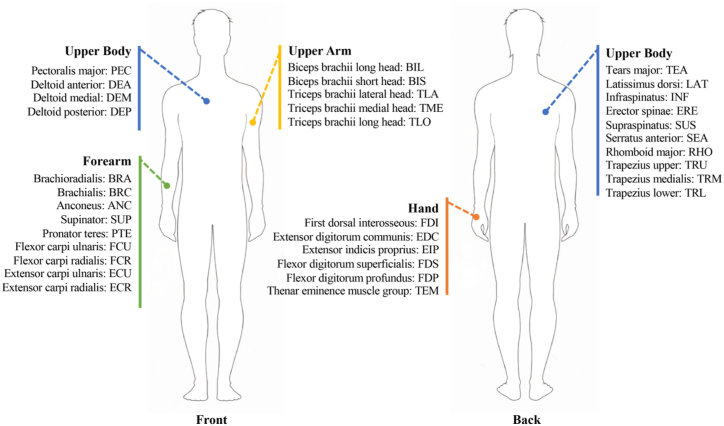
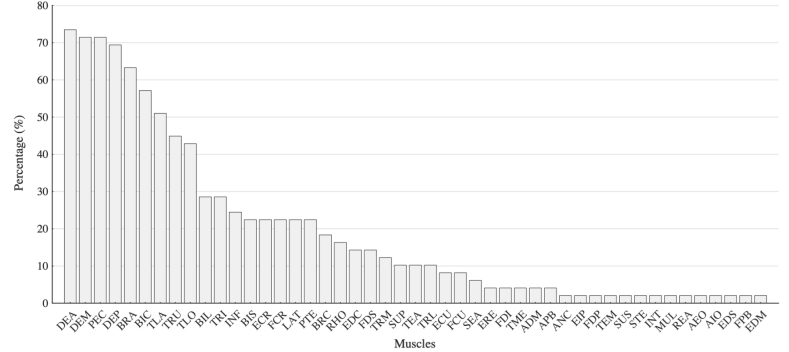
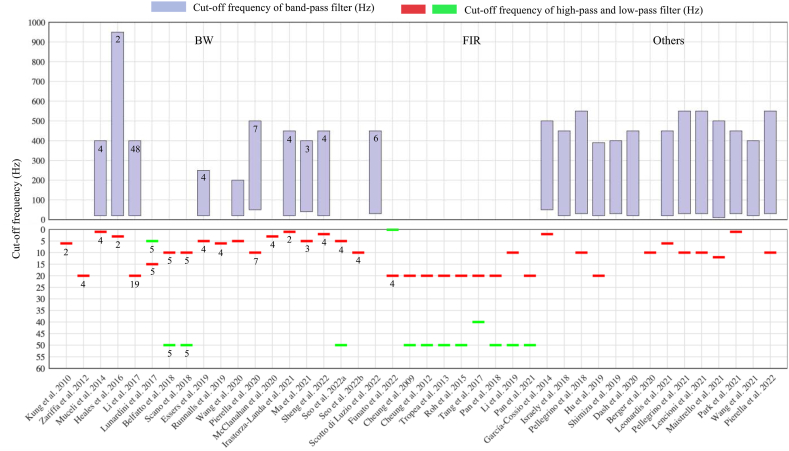
383 articles were screened and 51 were selected, which involved a total of 13 diseases and 748 patients and 1155 participants. Each study investigated on average 15 ± 10 patients. Four to forty-one muscles were included in the muscle synergy analysis. Point-to-point reaching was the most used task. The preprocessing of EMG signals and algorithms for synergy extraction varied among studies, and non-negative matrix factorization was the most used method. Five EMG normalization methods and five methods for identifying the optimal number of synergies were used in the selected papers. Most of the studies report that analyses on synergy number, structure, and activations provide novel insights on the physiopathology of motor control that cannot be gained with standard clinical assessments, and suggest that muscle synergies may be useful to personalize therapies and to develop new therapeutic strategies. However, in the selected studies synergies were used only for assessment; different testing procedures were used and, in general, study-specific modifications of muscle synergies were observed; single session or longitudinal studies mainly aimed at assessing stroke (71% of the studies), even though other pathologies were also investigated. Synergy modifications were either study-specific or were not observed, with few analyses available for temporal coefficients. Thus, several barriers prevent wider adoption of muscle synergy analysis including a lack of standardized experimental protocols, signal processing procedures, and synergy extraction methods. A compromise in the design of the studies must be found to combine the systematicity of motor control studies and the feasibility of clinical studies. There are however several potential developments that might promote the use of muscle synergy analysis in clinical practice, including refined assessments based on synergistic approaches not allowed by other methods and the availability of novel models. Finally, neural substrates of muscle synergies are discussed, and possible future research directions are proposed.
This review provides new perspectives about the challenges and open issues that need to be addressed in future work to achieve a better understanding of motor impairments and rehabilitative therapy using muscle synergies. These include the application of the methods on wider scales, standardization of procedures, inclusion of synergies in the clinical decisional process, assessment of temporal coefficients and temporal-based models, extensive work on the algorithms and understanding of the physio-pathological mechanisms of pathology, as well as the application and adaptation of synergy-based approaches to various rehabilitative scenarios for increasing the available evidence.
肌肉协同作用被认为是中枢神经系统用于控制运动的一种策略。肌肉协同分析是一个成熟的框架,用于研究神经疾病的病理生理基础,并且在过去几十年中已应用于临床应用的分析和评估,尽管它尚未在临床诊断、康复治疗和干预中广泛使用。即使研究结果存在不一致性,且缺乏包括信号处理和协同分析在内的规范流程限制了进展,但仍可识别出一些共同的发现和结果作为未来研究的基础。因此,需要一篇文献综述来总结先前关于临床环境中上肢肌肉协同作用的研究方法和主要发现,以便:i)总结目前的主要发现;ii)突出限制其在临床应用中使用的障碍;iii)提出促进将实验研究转化为临床场景所需的未来研究方向。
对使用肌肉协同作用来分析和评估神经功能障碍中上肢功能的文章进行综述。文献研究在Scopus、PubMed和Web of Science中进行。报告并讨论了实验方案(例如,研究目的、参与者数量和类型、肌肉数量和类型以及任务)、方法(例如,肌肉协同模型和协同提取方法、信号处理方法)以及符合条件的研究的主要发现。
筛选了383篇文章,选择了51篇,涉及总共13种疾病、748名患者和1155名参与者。每项研究平均调查15±10名患者。肌肉协同分析中包括4至41块肌肉。点对点伸手是最常用的任务。肌电图信号的预处理和协同提取算法在不同研究中有所不同,非负矩阵分解是最常用的方法。所选论文中使用了五种肌电图归一化方法和五种确定最佳协同数量的方法。大多数研究报告称,对协同数量、结构和激活的分析为运动控制的病理生理学提供了新的见解,而这些见解是通过标准临床评估无法获得的,并表明肌肉协同作用可能有助于个性化治疗和制定新的治疗策略。然而,在所选研究中,协同作用仅用于评估;使用了不同的测试程序,并且一般观察到针对特定研究的肌肉协同作用变化;单节段或纵向研究主要旨在评估中风(71%的研究),尽管也研究了其他病理情况。协同作用的变化要么是针对特定研究的,要么未被观察到,关于时间系数的分析很少。因此,几个障碍阻碍了肌肉协同分析的更广泛应用,包括缺乏标准化的实验方案、信号处理程序和协同提取方法。必须在研究设计中找到一种折衷方案,以结合运动控制研究的系统性和临床研究的可行性。然而,有几个潜在的发展方向可能会促进肌肉协同分析在临床实践中的应用,包括基于其他方法无法实现的协同方法的精细评估以及新模型的可用性。最后,讨论了肌肉协同作用的神经基础,并提出了可能的未来研究方向。
本综述为未来工作中需要解决的挑战和未解决问题提供了新的视角,以便更好地理解使用肌肉协同作用的运动障碍和康复治疗。这些包括在更广泛范围内应用这些方法、程序标准化、将协同作用纳入临床决策过程、评估时间系数和基于时间的模型、对算法进行大量研究以及理解病理的生理病理机制,以及将基于协同作用的方法应用和调整到各种康复场景以增加可用证据。