Baget-Bernaldiz Marc, Romero-Aroca Pedro, Bautista-Perez Angel, Mercado Joaquin
Ophthalmic Service, University Hospital Sant Joan, Reus, Spain.
Institut de Investigacio Sanitaria Pere Virgili [IISPV], University Rovira and Virgili, Tarragona, Spain.
Doc Ophthalmol. 2017 Oct;135(2):85-96. doi: 10.1007/s10633-017-9601-2. Epub 2017 Aug 4.
To determine the changes in the multifocal electroretinogram (mfERG) at 1 year in a clinical series of diabetic macular edema (DME) patients treated with ranibizumab (RNBZ) using a pro re nata protocol.
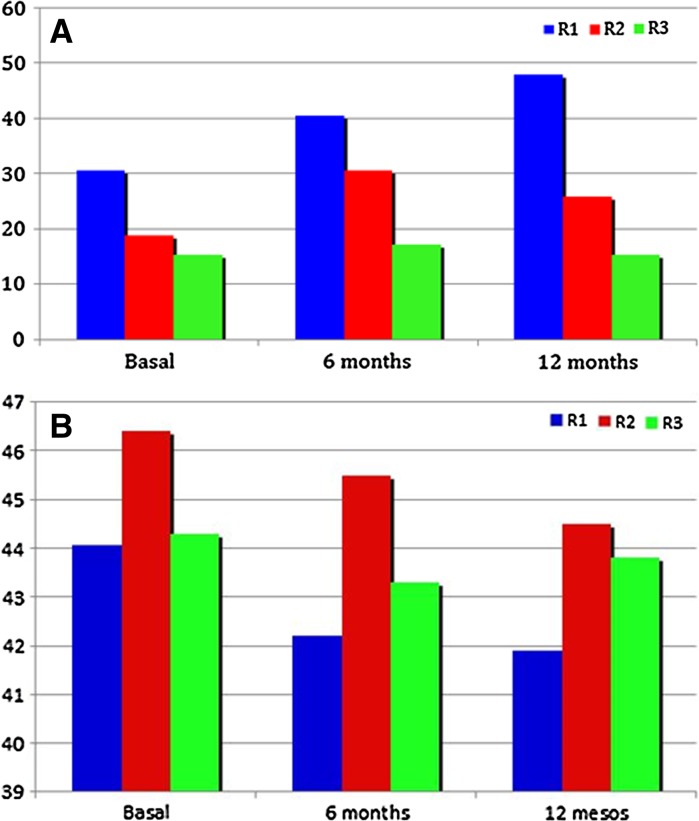
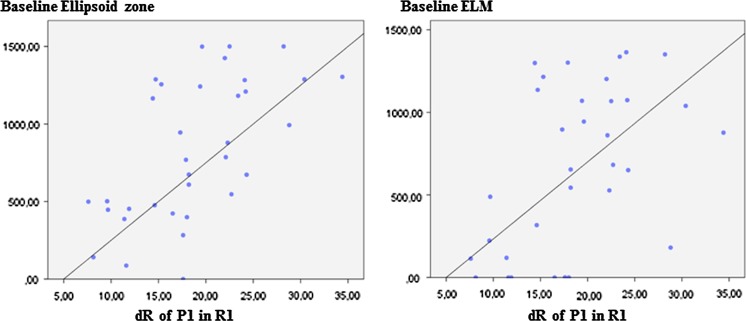
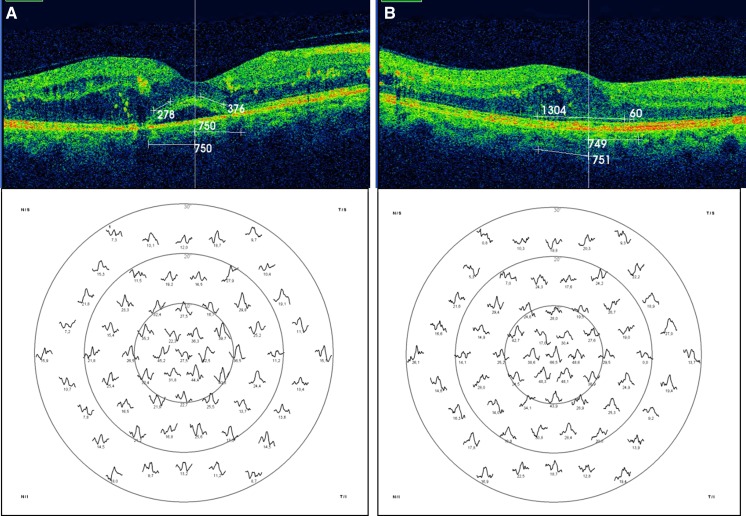
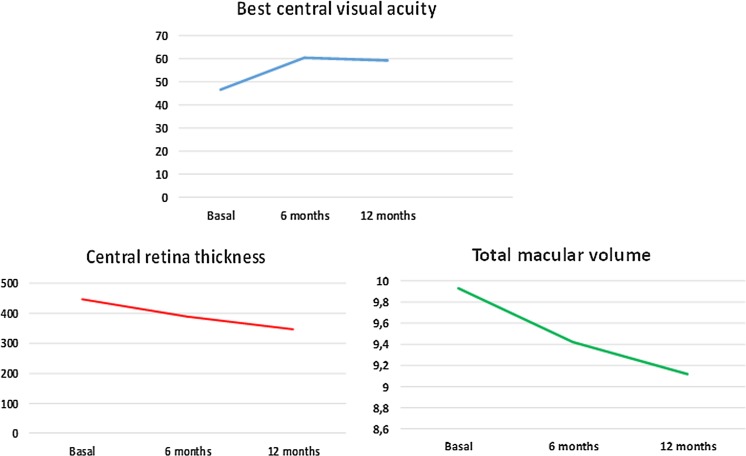
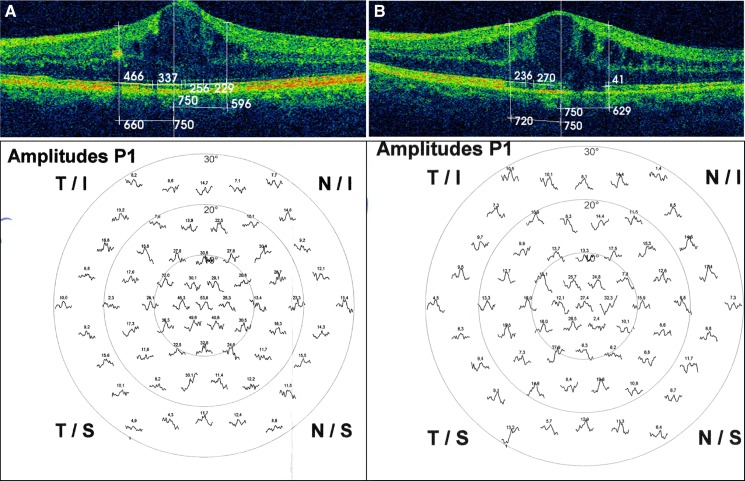
We analyzed a clinical series of 35 eyes of 35 patients with DME at baseline and after treating them with RNBZ over 1 year, in order to determine the change in the macular function, which was assessed by means of the response density and the implicit time of the first-order kernel (FOK) P1 wave of the mfERG at the foveola (R1), fovea (R2) and parafovea (R3). These electrophysiological parameters were studied taking into account different independent variables, such as DME type, degree of diabetic retinopathy (DR), level of preservation of both the ellipsoid zone (IS/OS) and the external limiting membrane (ELM) and changes in central retinal thickness (CRT) and total macular volume (TMV). We also studied the relationship between the response density and the best-corrected visual acuity (BCVA).
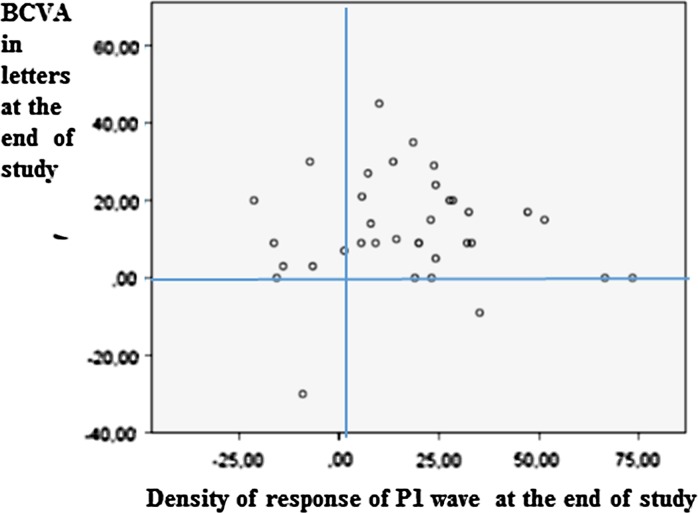
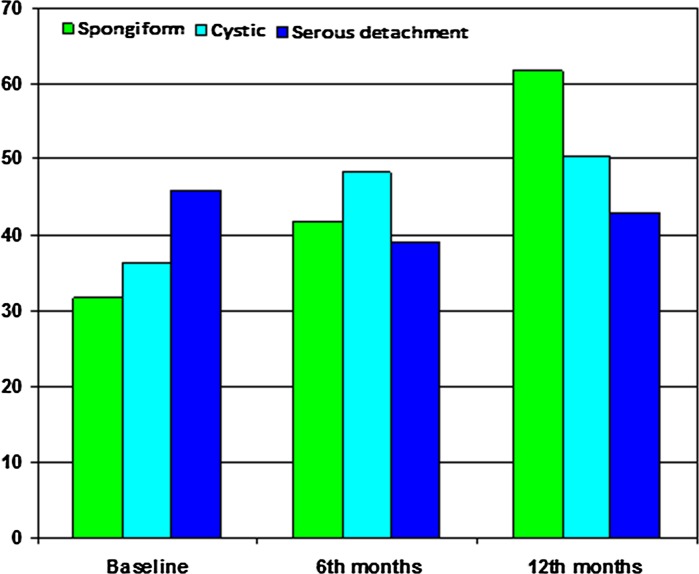
Eyes with cystic and spongiform DME showed better response density with respect to the serous type (p < 0.001) at baseline. Similarly, eyes with high IS/OS and ELM preservation rates showed higher initial response density compared to the others (p < 0.001). Eyes with moderate DR had better response density compared to those with severe and proliferative DR (p = 0.001). At the beginning of the study, those eyes with proliferative and severe DR showed longer implicit times with respect to those with moderate DR (p = 0.04). The response density significantly increased in eyes that anatomically restored the IS/OS and the ELM after being treated with RNBZ (both p < 0.001). Similarly, eyes with spongiform DME further improved the response density with respect to those with cystic and serous DME (p < 0.001). On the contrary, eyes with hard exudates showed less improvement in their response density at the end of the study (p < 0.001). We observed a significant relationship between BCVA and the response density achieved at the end of the study (p = 0.012). Eyes with severe and proliferative DR significantly shortened implicit time compared to those with moderate DR (p = 0.04).
The multifocal electroretinogram allowed us to differentiate groups of eyes with DME according to their electrophysiological profile, both initially and after being treated with RNBZ. Ranibizumab increased the response density in all DME types included in the study, with a maximum response in those eyes with spongiform type. Once treated with RNBZ, the macular electrophysiological activity improved in eyes that had a well-preserved ellipsoid zone and ELM. The presence of hard exudates was a limitation to the response density achieved at the foveola.
采用按需给药方案,确定雷珠单抗(RNBZ)治疗的糖尿病性黄斑水肿(DME)患者临床系列中1年时多焦视网膜电图(mfERG)的变化。
我们分析了35例DME患者的35只眼在基线时以及用RNBZ治疗1年后的情况,以确定黄斑功能的变化,通过mfERG在中心凹(R1)、黄斑中心凹(R2)和黄斑旁中心凹(R3)处的一阶核(FOK)P1波的反应密度和隐含时间进行评估。研究这些电生理参数时考虑了不同的独立变量,如DME类型、糖尿病视网膜病变(DR)程度、椭圆体带(IS/OS)和外界膜(ELM)的保存水平以及中心视网膜厚度(CRT)和黄斑总体积(TMV)的变化。我们还研究了反应密度与最佳矫正视力(BCVA)之间的关系。
在基线时,囊样和海绵状DME的眼相对于浆液性类型显示出更好的反应密度(p < 0.001)。同样,IS/OS和ELM保存率高的眼与其他眼相比,初始反应密度更高(p < 0.001)。中度DR的眼与重度和增殖性DR的眼相比,反应密度更好(p = 0.001)。在研究开始时,增殖性和重度DR的眼相对于中度DR的眼显示出更长的隐含时间(p = 0.04)。用RNBZ治疗后解剖学上恢复了IS/OS和ELM的眼中,反应密度显著增加(两者p < 0.001)。同样地,海绵状DME的眼相对于囊样和浆液性DME的眼,反应密度进一步改善(p < 0.001)。相反,有硬性渗出的眼在研究结束时反应密度改善较少(p < 0.001)。我们观察到BCVA与研究结束时达到的反应密度之间存在显著关系(p = 0.012)。重度和增殖性DR的眼与中度DR的眼相比,隐含时间显著缩短(p = 0.04)。
多焦视网膜电图使我们能够根据电生理特征在初始时以及用RNBZ治疗后区分DME的眼组。雷珠单抗增加了研究中包括的所有DME类型的反应密度,在海绵状类型的眼中反应最大。一旦用RNBZ治疗,椭圆体带和ELM保存良好的眼中黄斑电生理活动得到改善。硬性渗出的存在是中心凹处反应密度达到的一个限制因素。