Yang Xiao-Mei, Tu Guo-Wei, Zheng Ji-Li, Shen Bo, Ma Guo-Guang, Hao Guang-Wei, Gao Jian, Luo Zhe
Department of Critical Care Medicine, Zhongshan Hospital, Fudan University, Shanghai, 200032, People's Republic of China.
Department of Nursing, Zhongshan Hospital, Fudan University, Shanghai, People's Republic of China.
BMC Nephrol. 2017 Aug 7;18(1):264. doi: 10.1186/s12882-017-0667-6.
To investigate the impact of timing the initiation of renal replacement therapy (RRT) on clinical outcomes in critically ill patients with acute kidney injury (AKI), focusing on the randomized controlled trials (RCTs) in this field.
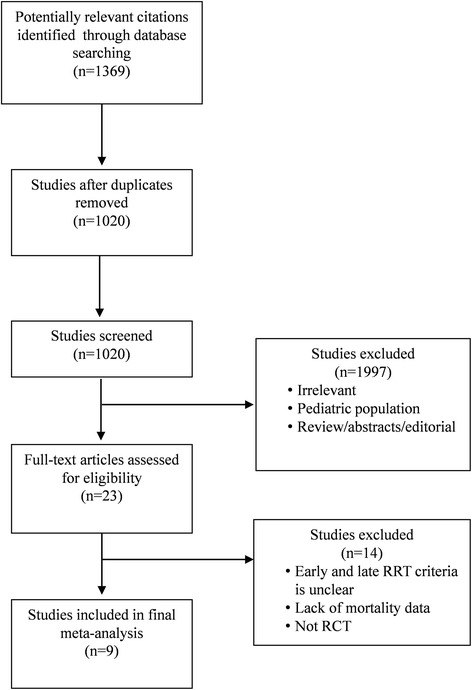
The PubMed, EMBASE and Cochrane databases were searched between January 1, 1985, and June 30, 2016, to identify randomized trials that assessed the timing of initiation of RRT in patients with AKI.
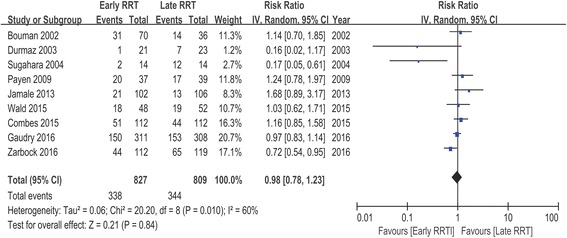
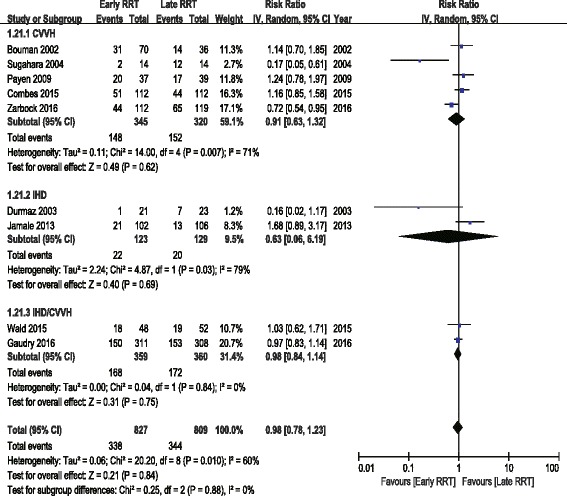
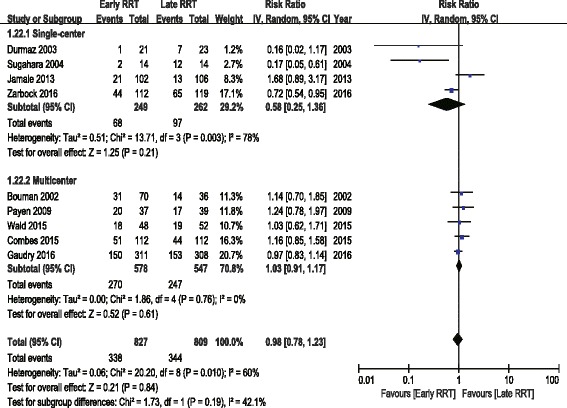
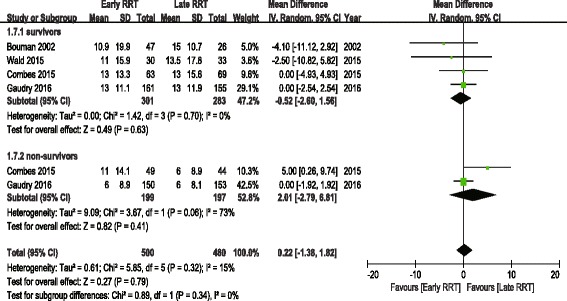
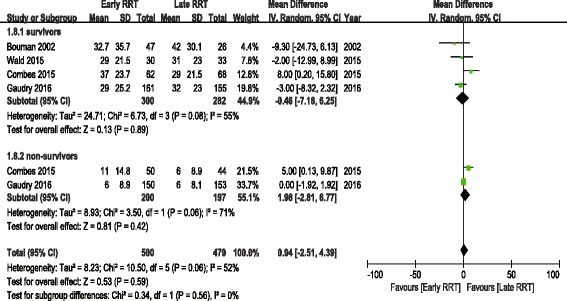
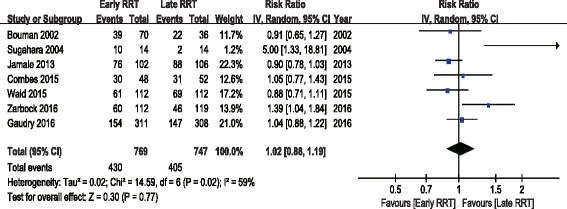
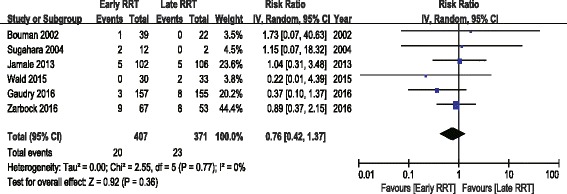
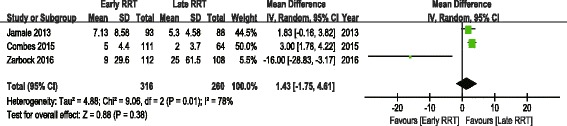
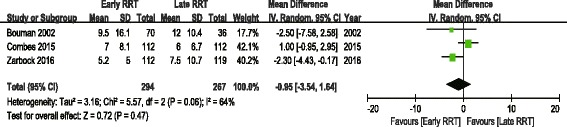
Nine RCTs, with a total of 1636 patients, were enrolled in this meta-analysis. A pooled analysis of the studies indicated no mortality benefit with "early" RRT, with an RR of 0.98 (95% CI 0.78 to 1.23, P = 0.84). There was no significant difference in intensive care unit (ICU) length of stay (LOS) or hospital LOS between the early and late RRT groups for survivors or nonsurvivors. Pooled analysis also demonstrated no significant change in renal function recovery (RR 1.02, 95% CI 0.88 to 1.19, I2 = 59%), RRT dependence (RR 0.76, 95% CI 0.42 to 1.37, I2 = 0%), duration of RRT (Mean difference 1.43, 95% CI -1.75 to 4.61, I2 = 78%), renal recovery time (Mean difference 0.73, 95% CI -2.09 to 3.56, I2 = 70%) or mechanical ventilation time (Mean difference - 0.95, 95% CI -3.54 to 1.64, I2 = 64%) between the early and late RRT groups. We found no significant differences in complications between the groups.
Our meta-analysis revealed that the "early" initiation of RRT in critically ill patients did not result in reduced mortality. Pooled analysis of secondary outcomes also showed no significant difference between the early and late RRT groups. More well-designed and large-scale trials are expected to confirm the result of this meta-analysis.
为研究开始肾脏替代治疗(RRT)的时机对急性肾损伤(AKI)危重症患者临床结局的影响,重点关注该领域的随机对照试验(RCT)。
检索1985年1月1日至2016年6月30日期间的PubMed、EMBASE和Cochrane数据库,以确定评估AKI患者开始RRT时机的随机试验。
本荟萃分析纳入了9项RCT,共1636例患者。对这些研究的汇总分析表明,“早期”RRT对死亡率无益处,风险比(RR)为0.98(95%置信区间[CI]为0.78至1.23,P = 0.84)。对于幸存者或非幸存者,早期和晚期RRT组在重症监护病房(ICU)住院时间(LOS)或医院LOS方面无显著差异。汇总分析还表明,早期和晚期RRT组在肾功能恢复(RR 1.02,95% CI 0.88至1.19,I² = 59%)、RRT依赖(RR 0.76,95% CI 0.42至1.37,I² = 0%)、RRT持续时间(平均差1.43,95% CI -1.75至4.61,I² = 78%)、肾脏恢复时间(平均差0.73,95% CI -2.09至3.56,I² = 70%)或机械通气时间(平均差 -0.95,95% CI -3.54至1.64,I² = 64%)方面无显著变化。我们发现两组之间并发症无显著差异。
我们的荟萃分析表明,危重症患者“早期”开始RRT并未降低死亡率。对次要结局的汇总分析也显示早期和晚期RRT组之间无显著差异。预计更多设计良好且大规模的试验将证实本荟萃分析的结果。