Entwisle Tom, Ling Yuan, Splatt Alex, Brukner Peter, Connell David
Imaging at Olympic Park, Melbourne, Victoria, Australia.
La Trobe University, Melbourne, Victoria, Australia.
Orthop J Sports Med. 2017 Jul 20;5(7):2325967117714998. doi: 10.1177/2325967117714998. eCollection 2017 Jul.
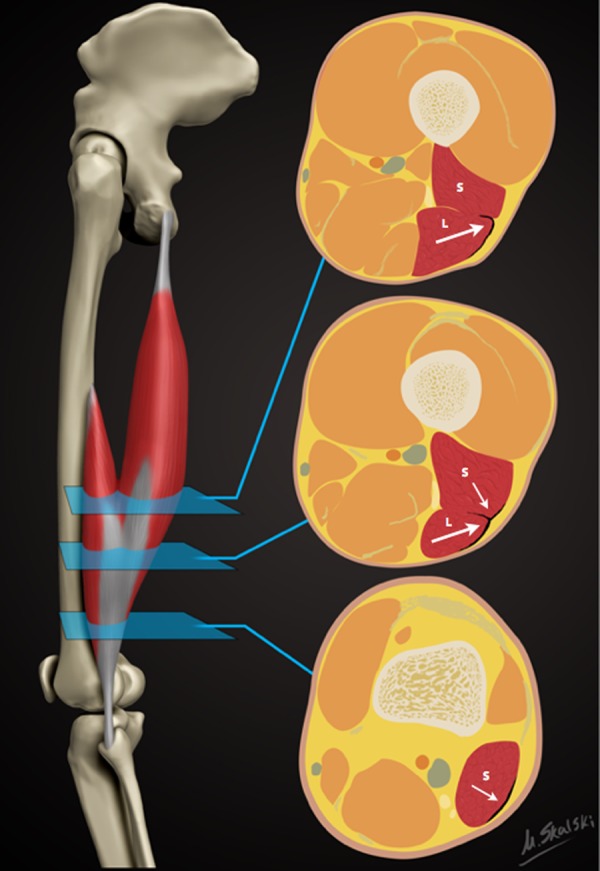
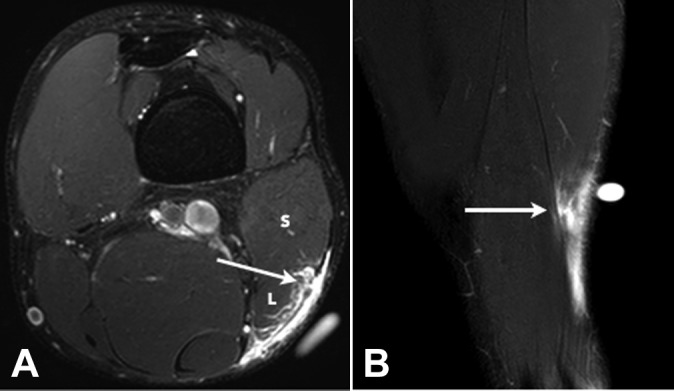
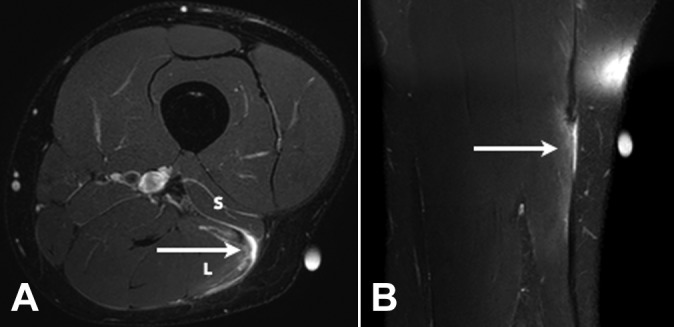
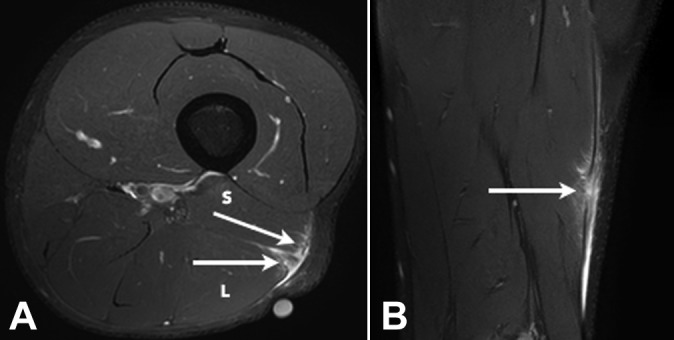
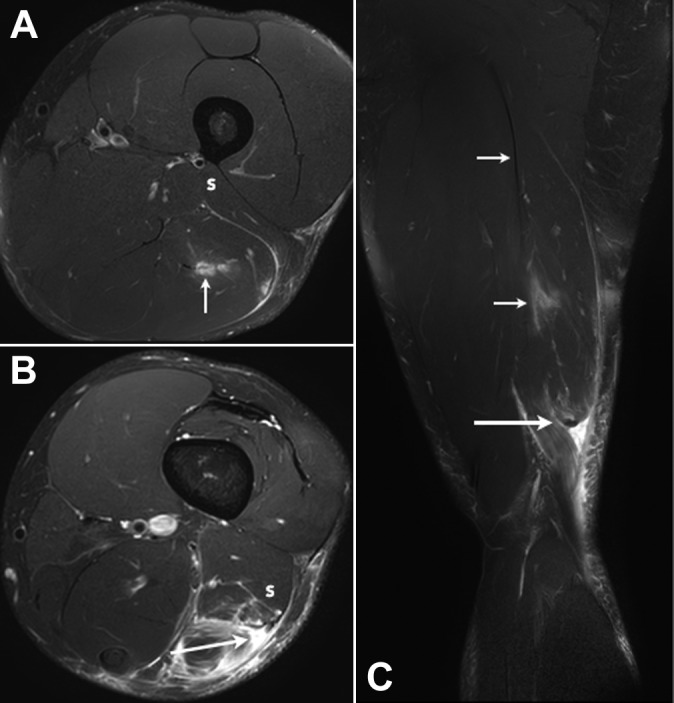
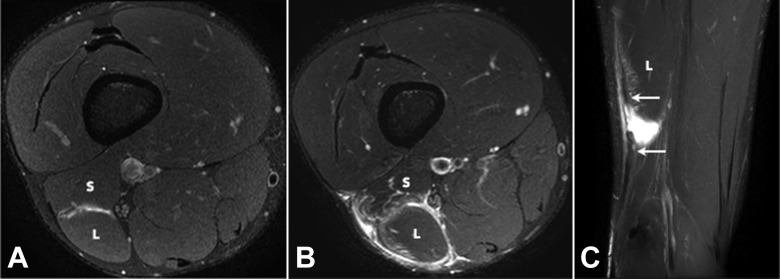
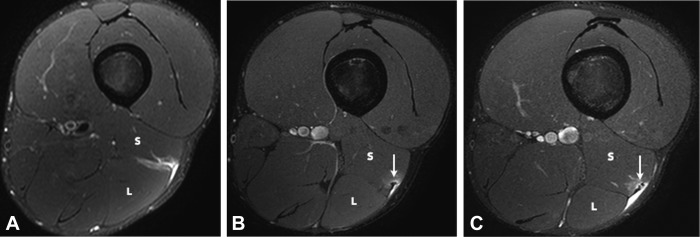
Injury to the distal musculotendinous T junction (DMTJ) of the biceps femoris is a distinct clinical entity that behaves differently from other hamstring injuries due to its complex, multicomponent anatomy and dual innervation. Injury in this region demonstrates a particularly high rate of recurrence, even with prolonged rehabilitation times.
To describe the anatomy of the DMTJ of the biceps femoris and analyze the injury patterns seen on magnetic resonance imaging (MRI) to aid prognosis and rehabilitation and minimize the risk of recurrence.
Cross-sectional study; Level of evidence, 3.
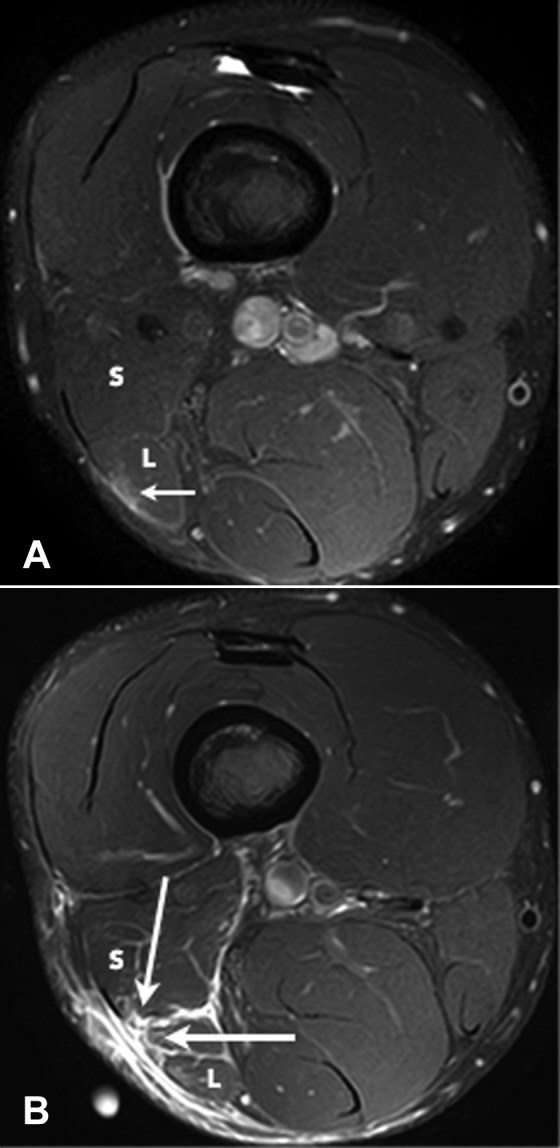
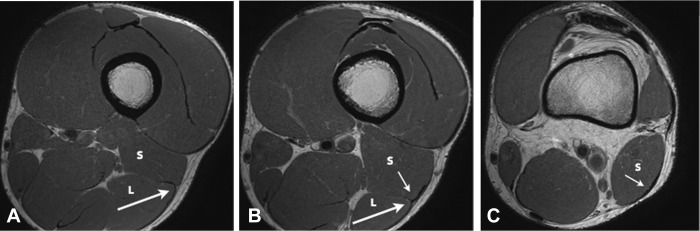
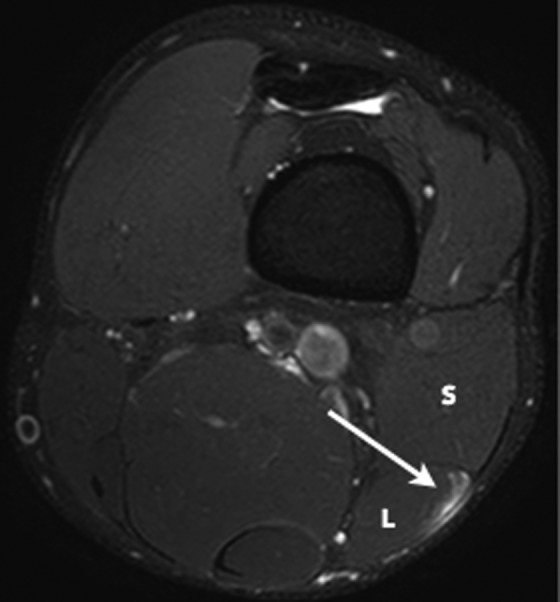
Acute injury to the DMTJ of the biceps femoris was identified in 106 MRI examinations from 55 patients at a single institution. Each injury was classified as involving the long head, the short head, or both components of the DMTJ, with each component individually graded. Injuries were classified as recurrent if there was a previous MRI demonstrating an acute injury to the DMTJ or if there was scarring present at the site of an acute injury.
Of the 106 acute injuries to the DMTJ of the biceps femoris, isolated injury to the long head component was the most common (51%), with both components involved in [round 42.5% to 43%] of cases. Isolated injury to the short head component accounted for 7% of cases. The recurrence rate for reinjury to the DMTJ was 54% in this series. The date of prior injury was known in 45 of 57 recurrent cases, with 34 of these reoccurring within 3 months (76%) and 40 reoccurring within 12 months (89%). The recurrent injury was of a higher grade than the prior injury in 22 of 44 instances (50%), the same grade in 16 instances (36%), and a lower grade in 6 instances (14%). Thus, 86% of recurrent injuries were of the same or higher grade than prior injury.
These results suggest that high-risk muscle injuries, such as that to the DMTJ of the biceps femoris, should be evaluated using MRI to determine the structural components involved and to assess the extent and severity of injury.
股二头肌远端肌腱肌肉交界处(DMTJ)损伤是一种独特的临床病症,由于其复杂的多成分解剖结构和双重神经支配,其表现与其他腘绳肌损伤不同。即使经过长时间的康复治疗,该区域损伤的复发率仍特别高。
描述股二头肌DMTJ的解剖结构,分析磁共振成像(MRI)所见的损伤模式,以辅助预后和康复,并将复发风险降至最低。
横断面研究;证据等级,3级。
在一家机构对55例患者的106次MRI检查中确定了股二头肌DMTJ的急性损伤。每次损伤分为累及DMTJ的长头、短头或两者,每个部分单独分级。如果之前的MRI显示DMTJ有急性损伤,或者急性损伤部位有瘢痕形成,则损伤被分类为复发性损伤。
在106例股二头肌DMTJ急性损伤中,长头部分单独损伤最为常见(51%),两者均受累的病例占[约42.5%至43%]。短头部分单独损伤占病例的7%。本系列中DMTJ再次损伤的复发率为54%。在57例复发病例中,45例知道先前损伤的日期,其中34例在3个月内复发(76%),40例在12个月内复发(89%)。在44例复发病例中,22例(50%)再次损伤的分级高于先前损伤,16例(36%)分级相同,6例(14%)分级较低。因此,86%的复发性损伤与先前损伤的分级相同或更高。
这些结果表明,对于高风险的肌肉损伤,如股二头肌DMTJ损伤,应使用MRI进行评估,以确定受累的结构成分,并评估损伤的范围和严重程度。