Department of Anaesthesiology and Intensive Care Medicine, Hannover Medical School, Carl-Neuberg-Str. 1, 30625, Hannover, Germany.
Trauma Department, Hannover Medical School, Carl-Neuberg-Str. 1, 30625, Hannover, Germany.
Eur J Med Res. 2017 Aug 10;22(1):27. doi: 10.1186/s40001-017-0268-7.
Videolaryngoscopy has been proven to be a safe procedure managing difficult airways in the hands of airway specialists. Information about the success rates in unexperienced users of videolaryngoscopy compared to conventional laryngoscopy is sparse. Therefore, we aimed to evaluate if there might be more success in securing an airway if the unexperienced provider is using a videolaryngoscope in simulated airways in a randomized manikin study. Differences between commonly used videolaryngoscopes were elucidated.
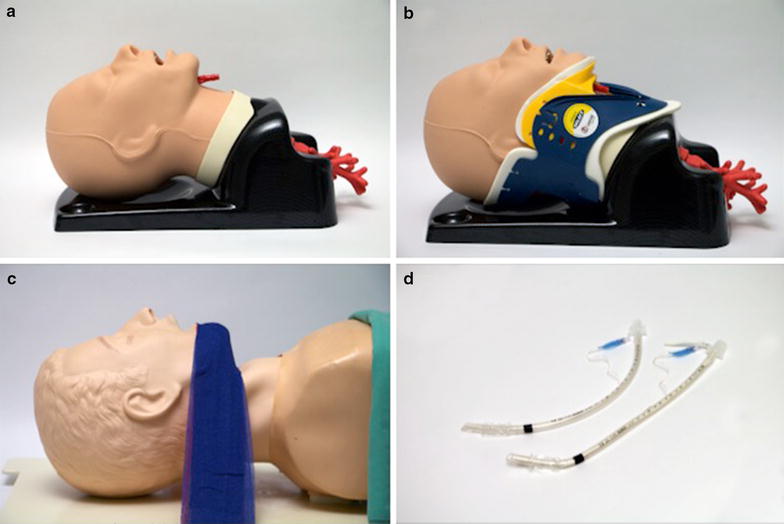
A standardized hands-on workshop prior to the study was performed. For direct laryngoscopy (DL) we used a Macintosh laryngoscope, whereas for videolaryngoscopy (VL) we used the cMac, the dBlade, and a King Vision videolaryngoscope. Endotracheal intubations in three simulated normal and difficult airways were performed. Main outcome parameters were time to view and time to intubation. Cormack and Lehane (C + L) classification and the percentage of glottic opening (POGO) score were evaluated. After every intubation, the participants were asked to review the airway and the device used.
22 participants (14.8 ± 4.0 intubations per year, mostly trauma surgeons) with limited experience in videolaryngoscopy (mean total number of videolaryngoscopy .4 ± .2) were enrolled. We found improved C + L grades with VL in contrast to DL. We saw similar data with respect to the POGO score, where the participants achieved better visibility of the glottis with VL. The hyperangulated blade geometries of videolaryngoscopes provided a better visibility in difficult airways than the standard geometry of the Macintosh-type blade. The subjective performance of the VL devices was better in more difficult airway scenarios.
After a short introduction and hands-on training, a videolaryngoscope seems to be safe and usable by unexperienced providers. We assume a standard geometry laryngoscope is optimal for a patient with normal anatomy, whereas VL device with a hyperangulated blade is ideal for difficult airway situations with limited mouth opening or restricted neck movement.
在气道专家手中,视频喉镜已被证明是一种安全的处理困难气道的方法。关于未经训练的使用者使用视频喉镜与传统喉镜相比成功率的信息很少。因此,我们旨在评估如果未经训练的提供者在模拟气道中使用视频喉镜是否可以更成功地确保气道,这是一项随机模拟人体研究。阐明了常用视频喉镜之间的差异。
在研究之前进行了标准化的实践操作研讨会。对于直接喉镜(DL),我们使用 Macintosh 喉镜,而对于视频喉镜(VL),我们使用 cMac、dBlade 和 King Vision 视频喉镜。在三个模拟正常和困难气道中进行了气管内插管。主要的结果参数是观察时间和插管时间。评估了 Cormack 和 Lehane(C + L)分类和声带开口百分比(POGO)评分。每次插管后,参与者被要求检查气道和使用的设备。
共有 22 名参与者(每年平均进行 4.0 ± 4.0 次插管,主要是创伤外科医生),他们在视频喉镜方面经验有限(平均总视频喉镜次数为.4 ±.2)。我们发现 VL 与 DL 相比,C + L 分级有所改善。在 POGO 评分方面,我们也看到了类似的数据,即参与者使用 VL 可以更好地观察声带。与 Macintosh 型刀片的标准几何形状相比,视频喉镜的超角刀片几何形状提供了更好的困难气道可视性。在更困难的气道情况下,VL 设备的主观性能更好。
经过简短的介绍和实践培训,视频喉镜似乎可以由未经训练的人员安全使用。我们假设标准几何形状的喉镜对解剖结构正常的患者是最佳的,而具有超角刀片的 VL 设备对于张口受限或颈部运动受限的困难气道情况是理想的。