Department of Medicine, Division of Nephrology, University of Alabama at Birmingham, Birmingham, Alabama.
Veterans Affairs Medical Center, Birmingham, Alabama; and.
Clin J Am Soc Nephrol. 2017 Nov 7;12(11):1823-1830. doi: 10.2215/CJN.01410217. Epub 2017 Aug 10.
The optimal type of initial permanent access for hemodialysis among the elderly is controversial. Duration of central venous catheter dependence, patient comorbidities, and life expectancy are important considerations in whether to place an arteriovenous fistula or graft. We used an observational study design to compare clinical outcomes in elderly patients who initiated hemodialysis with a central venous catheter and subsequently had an arteriovenous fistula or graft placed.
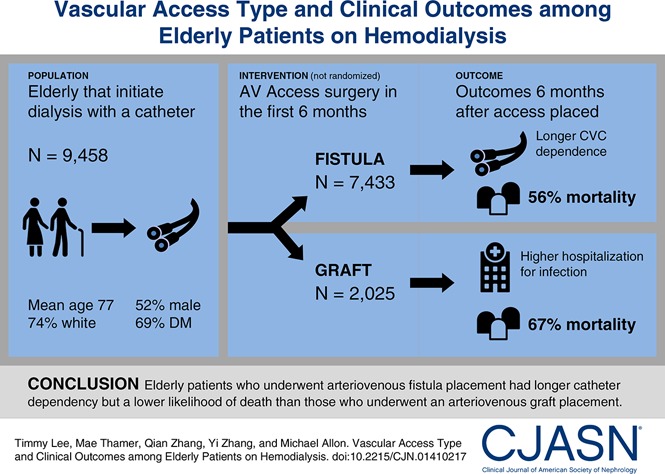
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We identified 9458 United States patients ages ≥67 years old who initiated hemodialysis from July 1, 2010 to June 30, 2011 with a central venous catheter and no secondary vascular access and then received an arteriovenous fistula (=7433) or graft (=2025) within 6 months. We evaluated key clinical outcomes during the 6 months after vascular access placement coincident with high rates of catheter use and used a matched propensity score analysis to examine patient survival.
Central venous catheter dependence was greater in every month during the 6-month period after arteriovenous fistula versus graft placement (<0.001). However, rates of all-cause infection-related hospitalization (adjusted relative risk, 0.93; 95% confidence interval, 0.87 to 0.99; =0.01) and bacteremia/septicemia-related hospitalization (adjusted relative risk, 0.90; 95% confidence interval, 0.82 to 0.98; =0.02) were lower in the arteriovenous fistula versus graft group as was the adjusted risk of death (hazard ratio, 0.76; 95% confidence interval, 0.73 to 0.80; <0.001).
Despite extended central venous catheter dependence, elderly patients initiating hemodialysis with a central venous catheter who underwent arteriovenous fistula placement within 6 months had fewer hospitalizations due to infections and a lower likelihood of death than those receiving an arteriovenous graft.
对于老年人,永久性初始血液透析通路的最佳类型存在争议。中心静脉导管依赖的持续时间、患者合并症和预期寿命是决定是否放置动静脉瘘或移植物的重要考虑因素。我们采用观察性研究设计,比较了在开始血液透析时使用中心静脉导管,随后在 6 个月内放置动静脉瘘或移植物的老年患者的临床结局。
设计、设置、参与者和测量:我们确定了 9458 名年龄≥67 岁的美国患者,他们于 2010 年 7 月 1 日至 2011 年 6 月 30 日期间开始血液透析,使用中心静脉导管,没有二级血管通路,随后在 6 个月内接受动静脉瘘(=7433)或移植物(=2025)。我们评估了血管通路放置后 6 个月内的关键临床结局,这一时期中心静脉导管的使用率较高,并使用匹配倾向评分分析来检查患者的生存情况。
与移植物相比,动静脉瘘放置后 6 个月内每个月的中心静脉导管依赖程度都更高(<0.001)。然而,所有原因感染相关住院率(调整后的相对风险,0.93;95%置信区间,0.87 至 0.99;=0.01)和菌血症/败血症相关住院率(调整后的相对风险,0.90;95%置信区间,0.82 至 0.98;=0.02)在动静脉瘘组中较低,调整后的死亡风险也较低(风险比,0.76;95%置信区间,0.73 至 0.80;<0.001)。
尽管中心静脉导管依赖时间延长,但开始血液透析时使用中心静脉导管的老年患者,如果在 6 个月内进行动静脉瘘放置,其感染相关住院率和死亡率均低于接受动静脉移植物的患者。