Moryoussef Frédérick, Sportes Adrien, Leblanc Sarah, Bachet Jean Baptiste, Chaussade Stanislas, Prat Frédéric
Department of Gastro-Enterology, La Pitié Salpetrière Teaching Hospital, AP-HP, Université Pierre et Marie Curie, Paris, France.
Department of Gastro-Enterology, Cochin Teaching Hospital, AP-HP, Université Paris Descartes, Sorbonne Paris Cite, Paris, France.
Therap Adv Gastroenterol. 2017 Jul;10(7):537-544. doi: 10.1177/1756283X17702614. Epub 2017 Apr 20.
Results of endoscopic ultrasound-guided biliary drainage (EUBD) are unknown in case of proximal stricture. The aim is to assess clinical outcomes of EUBD in patients with malignant hilar obstruction.
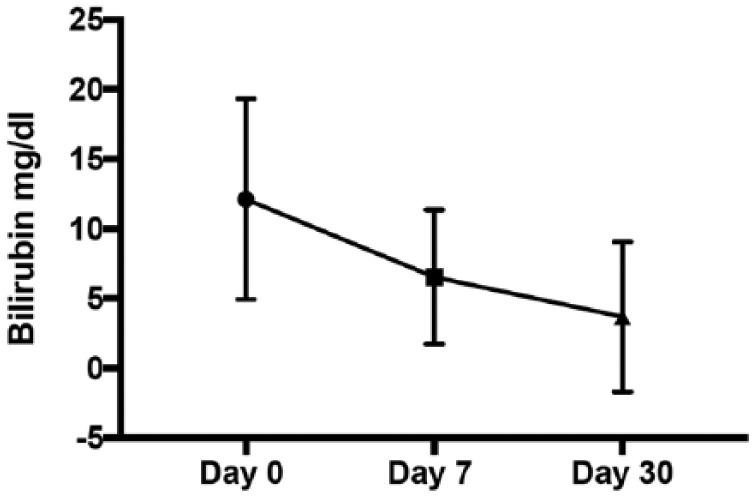
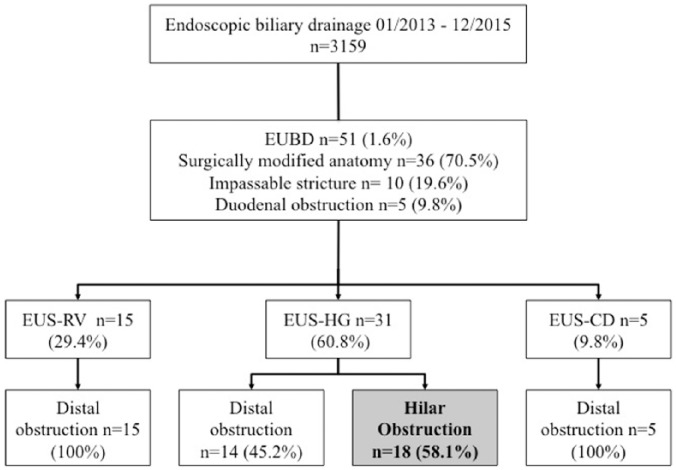
Patients undergoing EUBD with hilar strictures were prospectively included. Primary outcome was clinical success at 7 and 30 days (defined by 50% bilirubin decrease). Secondary outcomes were technical success, procedure-related complications, length of hospital stay, reintervention rate, survival and chemotherapy administration.
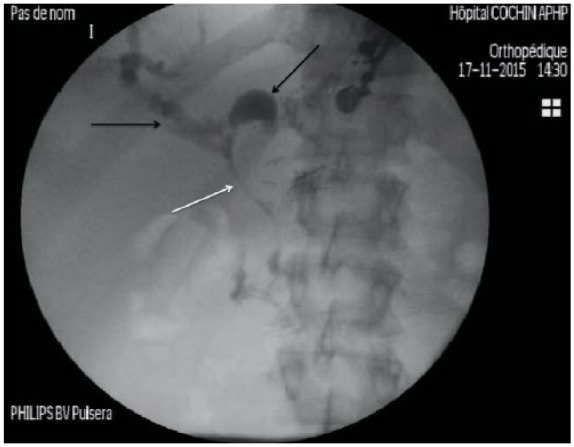
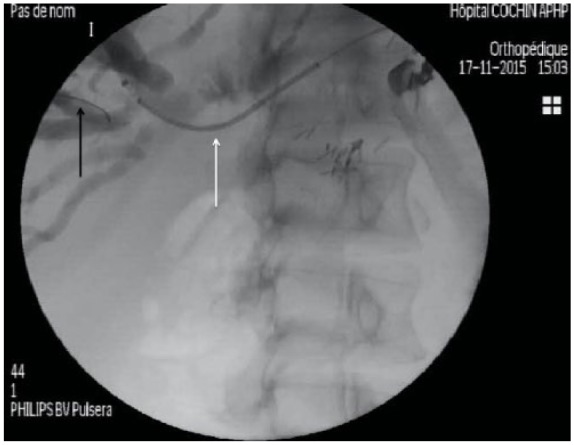
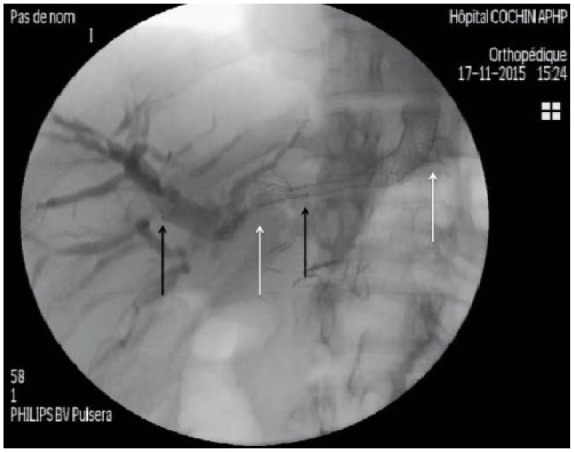
Eighteen patients with a mean age of 68.8 years were included. On 15 classable stenosis, 7 (47%) were noted Bismuth I-II, 7 (47%) Bismuth III, and 1 (6.7%) Bismuth IV. Reasons for EUBD were surgically modified anatomy in 10 patients (55.6%), impassable stricture at ERCP in 7 (38.9%) and duodenal obstruction in 1 (5.6%). Only hepaticogastrostomy was performed. Clinical success was at day 7 and 30 respectively 72.2% and 68.8%. Technical success was 94%. Complications occurred in 3 (16.7%) patients. Median (range) length of hospital stay was 10 (6-35) days. Reintervention rate was 16.7%. Median (range) survival was 79 (5-390) days. Chemotherapy was possible in 10 (55.6%) patients.
EUBD is feasible for hilar obstruction for surgically altered anatomy or after ERCP failure. Clinical outcome is satisfactory when considering underlying advanced disease, allowing chemotherapy.
对于近端狭窄,内镜超声引导下胆道引流(EUBD)的结果尚不清楚。目的是评估EUBD在恶性肝门梗阻患者中的临床疗效。
前瞻性纳入接受EUBD治疗肝门狭窄的患者。主要结局是7天和30天时的临床成功(定义为胆红素降低50%)。次要结局包括技术成功、与操作相关的并发症、住院时间、再次干预率、生存率和化疗给药情况。
纳入18例平均年龄68.8岁的患者。在15例可分类的狭窄中,7例(47%)为Bismuth I-II型,7例(47%)为Bismuth III型,1例(6.7%)为Bismuth IV型。EUBD的原因包括10例(55.6%)手术改变解剖结构、7例(38.9%)ERCP时狭窄无法通过和1例(5.6%)十二指肠梗阻。仅进行了肝胃吻合术。7天和30天时的临床成功率分别为72.2%和68.8%。技术成功率为94%。3例(16.7%)患者发生并发症。中位(范围)住院时间为10(6 - 35)天。再次干预率为16.7%。中位(范围)生存期为79(5 - 390)天。10例(55.6%)患者可行化疗。
对于手术改变解剖结构或ERCP失败后的肝门梗阻,EUBD是可行的。考虑到潜在的晚期疾病,临床结局令人满意,且允许进行化疗。