Nicholls Luke, Winter Amber, Harwood Ashley, Plank Ashley, Bagga Preeti, Wong Winnie, Khoo Eric
Radiation Oncology Centres, St Andrews Cancer Care, Toowoomba, Queensland, Australia.
School of Medicine, University of Queensland, St Lucia, Brisbane, Queensland, Australia.
J Med Radiat Sci. 2017 Dec;64(4):259-265. doi: 10.1002/jmrs.240. Epub 2017 Aug 14.
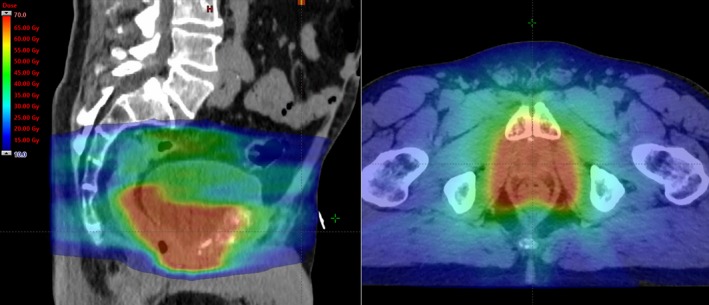
To investigate the efficacy and toxicity of radiation therapy (RT) after radical prostatectomy (RP) for prostate cancer at Radiation Oncology Centres, Toowoomba.
The electronic medical records of 130 consecutive patients with histologically proven prostate adenocarcinoma who underwent post-prostatectomy RT between January 2008 and December 2014 were analysed. Primary endpoint was Biochemical Recurrence (BCR) after RT. BCR was defined by PSA > 0.2 ng/mL and BCR endpoints were analysed using Kaplan-Meier methods. The impact of RT technique and the rates of acute and late toxicities are also reported. Toxicities were graded according to Radiation Therapy Oncology Group (RTOG) criteria.
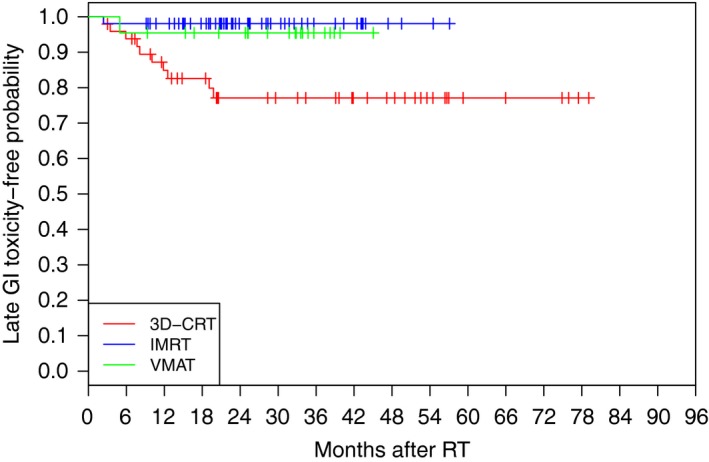
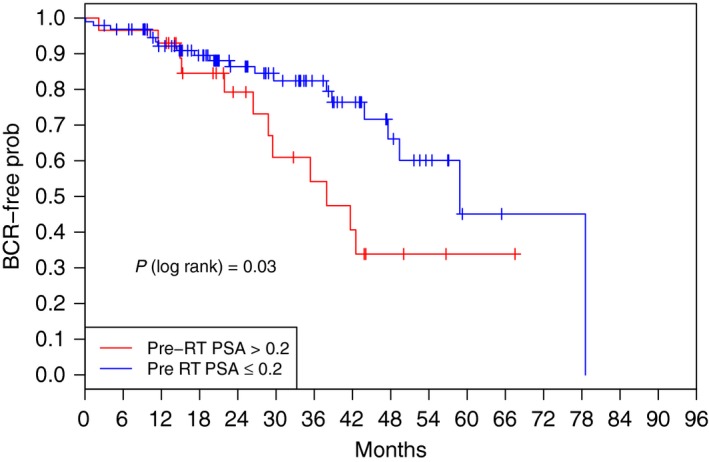
Median follow-up time after RT (regardless of technique) was 28 months. BCR occurred in 32 of the 126 patients (25%) whose prostate specific antigen (PSA) levels have been monitored post-RT. At 24 and 36 months, 85% and 75% of patients were BCR-free, respectively. Patients with a pre-RT PSA above 0.2 ng/mL had a higher probability of recurrence than patients with values below 0.2 ng/mL (P = 0.03). RT technique, pelvic nodal irradiation, androgen deprivation therapy, T staging or surgical margin did not significantly impact BCR results. No patient experienced acute toxicities greater than grade 2. Grade 1 or 2 late gastrointestinal (GI) toxicity occurred in 11% and 1 patient experienced a grade 3 event. 12% of patients developed grade 1 or 2 late genitourinary (GU) toxicity, with evidence of grade 3 severity in only 1 patient. Evidence of a trend in reduction in late GI toxicity with the use of intensity modulated radiation therapy (IMRT) or volumetric modulated arc therapy (VMAT) was apparent but not with late GU toxicity.
At our regional centre, early RT (PSA < 0.2 ng/mL) was associated with significant improvement in BCR-free survival. Rates of toxicity mirror those of landmark trials which suggest no detriment for our regional prostate cancer patients. The use of IMRT/VMAT techniques was associated with a trend towards reduced rates of GI toxicity.
在图文巴放射肿瘤中心,研究前列腺癌根治性前列腺切除术后放射治疗(RT)的疗效和毒性。
分析了2008年1月至2014年12月期间连续130例经组织学证实为前列腺腺癌且接受前列腺切除术后放疗患者的电子病历。主要终点是放疗后的生化复发(BCR)。BCR定义为前列腺特异性抗原(PSA)>0.2 ng/mL,并使用Kaplan-Meier方法分析BCR终点。还报告了放疗技术的影响以及急性和晚期毒性发生率。毒性根据放射治疗肿瘤学组(RTOG)标准分级。
放疗后(无论技术如何)的中位随访时间为28个月。在放疗后监测前列腺特异性抗原(PSA)水平的126例患者中,有32例(25%)发生了BCR。在24个月和36个月时,分别有85%和75%的患者无BCR。放疗前PSA高于0.2 ng/mL的患者比低于0.2 ng/mL的患者复发概率更高(P = 0.03)。放疗技术、盆腔淋巴结照射、雄激素剥夺治疗、T分期或手术切缘对BCR结果无显著影响。没有患者经历大于2级的急性毒性。11%的患者发生1级或2级晚期胃肠道(GI)毒性,1例患者发生3级事件。12%的患者出现1级或2级晚期泌尿生殖系统(GU)毒性,只有1例患者有3级严重程度的证据。使用调强放射治疗(IMRT)或容积调强弧形治疗(VMAT)后晚期GI毒性有降低趋势,但晚期GU毒性不明显。
在我们的地区中心,早期放疗(PSA < 0.2 ng/mL)与无BCR生存率的显著提高相关。毒性发生率与标志性试验相似,表明对我们地区的前列腺癌患者没有不利影响。IMRT/VMAT技术的使用与GI毒性发生率降低的趋势相关。