Department of Psychiatry and Neurology & Ophthalmology, Michigan State University, East Lansing, MI, USA.
Centre NeuroPsychopathologique (CNPP), University of Kinshasa, Kinshasa, Congo.
Lancet Glob Health. 2017 Sep;5(9):e936-e947. doi: 10.1016/S2214-109X(17)30267-X.
Konzo is an irreversible upper-motor neuron disorder affecting children dependent on bitter cassava for food. The neurocognitive ability of children with konzo over time has yet to be fully documented.
We did a longitudinal study in a konzo outbreak zone continuously affected by konzo since 1990, in the district of Kahemba, southern Bandundu Province, Congo. We enrolled children with a record of neurological diagnosis of konzo in Kahemba town. For all study children with konzo enrolled in the final sample for the baseline assessment, a neurological exam was done by neurologists to confirm konzo diagnosis using the 1996 WHO criteria at 2 years and 4 years. In the initial baseline sample for each child with konzo, we attempted to get consent from a comparison child without konzo (1996 WHO criteria) within 2 years of age, from a neighbouring household who met inclusion criteria. The neuropsychological assessments were the Kaufman Assessment Battery for Children, second edition (KABC-II), and the Bruininks-Oseretsky Test of Motor Proficiency, second edition (BOT-2).
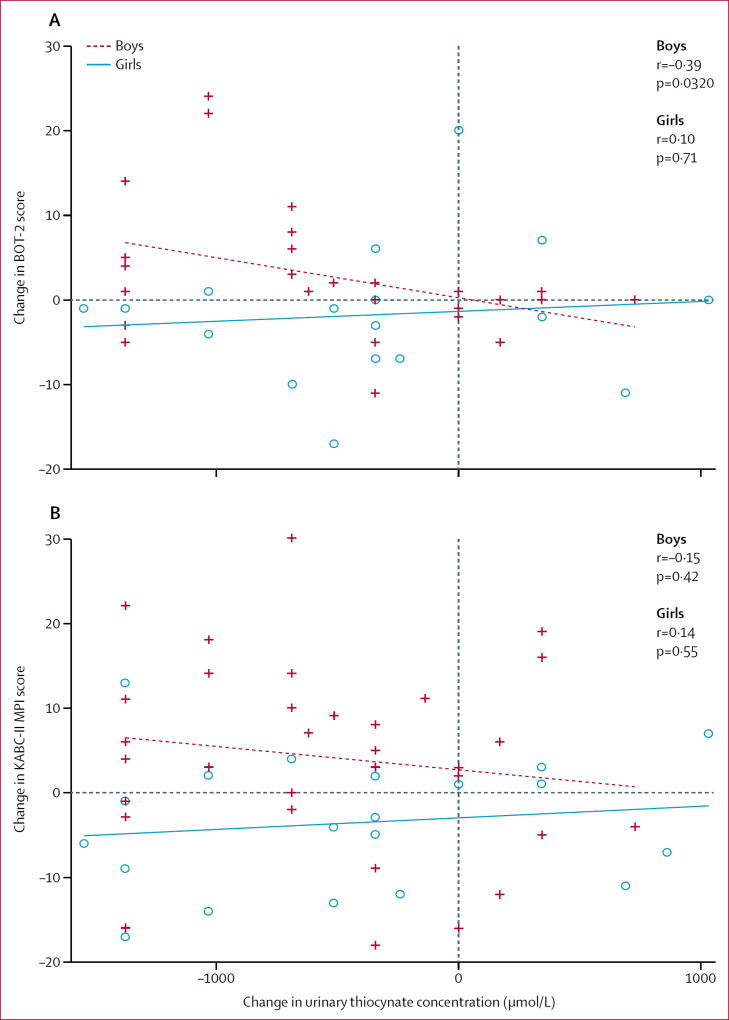
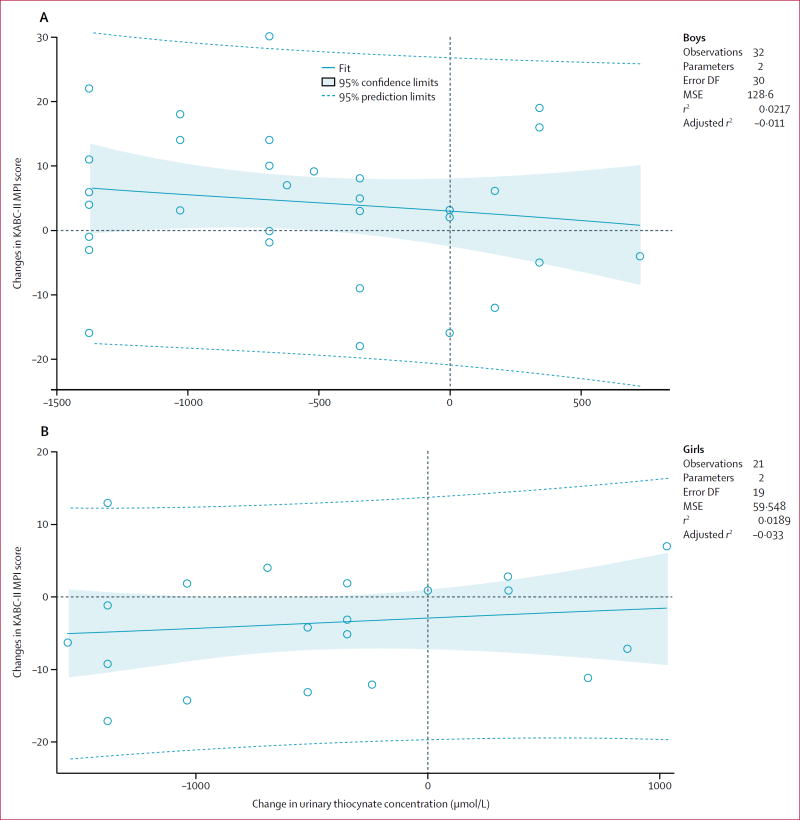
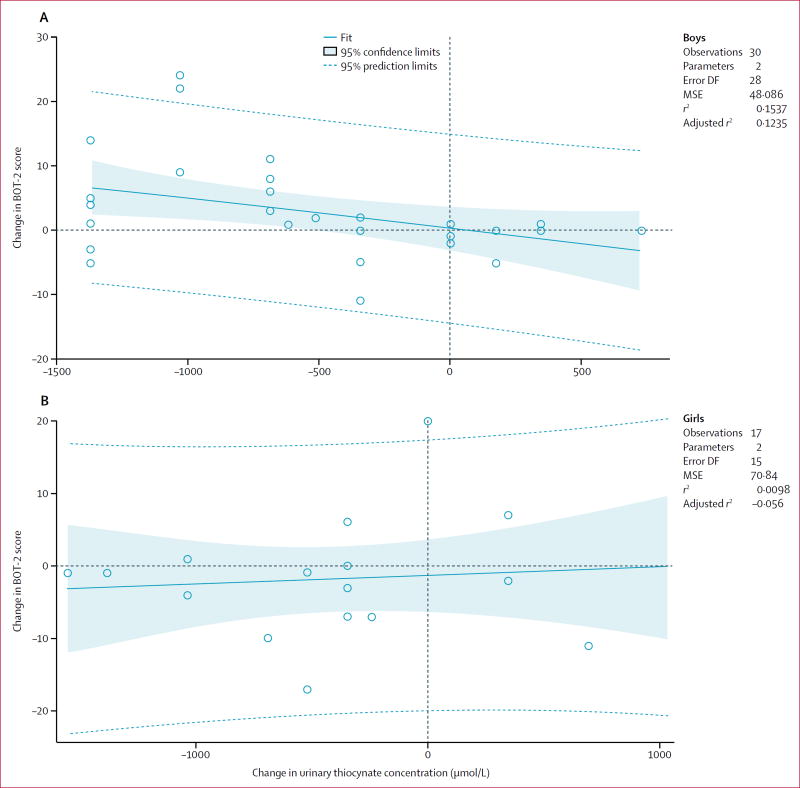
Data collection occurred between Oct 12, 2011, and Aug 14, 2015, in the town of Kahemba. 123 children from the Congo with konzo and 87 presumably healthy children without konzo from neighbouring households were enrolled. The planned assessments were completed by 76 children with konzo and 82 children without konzo at 2-year follow-up, and by 55 children with konzo and 33 children without konzo at 4-year follow-up. Boys with konzo did worse than those without konzo on the KABC-II Learning (p=0·0424) and on the Mental Processing Index (MPI; p=0·0111) assessments at 2-year follow-up, but girls did not. These differences observed in boys might have been caused by stunting. At 4-year follow-up, the difference in KABC-II MPI score between boys or girls with or without konzo was not significant. Both boys and girls with konzo had lower scores on BOT-2 than children without konzo at both follow-up times (p<0·0001). These differences were not attenuated when controlling for physical growth. Boys with and without konzo declined on BOT-2 fine motor proficiency at 2-year follow-up (boys with konzo p=0·0076; boys without konzo p=0·0224) and KABC-II MPI performance at 2-year follow-up and 4-year follow-up (2 years: boys with konzo p<0·0001, boys without konzo p=0·0213; 4 years: boys with konzo p=0·0256, boys without konzo p=0·10), but that was not the case for the girls with scores remaining stable regardless of konzo status. For boys, increases in urinary thiocyanate concentration was significantly associated with reductions in BOT-2 motor proficiency (p=0·0321), but was not significantly associated in girls and urinary thiocyanate concentration was not associated with KABC-II MPI score for either boys or girls.
Motor and cognitive performance continues to be significantly impaired in boys with konzo at 2-year follow-up compared with boys without konzo. Because these impairments are associated in part with exposure to poorly processed cassava as measured by urinary thiocyanate, interventions are urgently needed to ensure improved processing of cassava to detoxify this food source.
US National Institutes of Health.
科酮病是一种不可逆的上运动神经元疾病,影响依赖苦木薯作为食物的儿童。患有科酮病的儿童的神经认知能力尚未得到充分记录。
我们在刚果南部班顿杜省卡亨巴区进行了一项纵向研究,该地区自 1990 年以来一直持续受到科酮病的影响。我们招募了在卡亨巴镇有科酮病神经学诊断记录的儿童。对于最终纳入基线评估的所有患有科酮病的研究儿童,神经病学家通过使用 1996 年世卫组织标准进行神经检查,在 2 岁和 4 岁时确认科酮病诊断。在每个患有科酮病的儿童的初始基线样本中,我们试图从年龄在 2 岁以内的、来自符合纳入标准的相邻家庭的无科酮病(1996 年世卫组织标准)的对照儿童那里获得同意。神经心理评估是 Kaufman 儿童评估量表,第二版(KABC-II)和 Bruininks-Oseretsky 运动技能测试,第二版(BOT-2)。
数据收集于 2011 年 10 月 12 日至 2015 年 8 月 14 日在卡亨巴镇进行。来自刚果的 123 名患有科酮病的儿童和来自相邻家庭的 87 名可能没有患有科酮病的健康儿童被纳入研究。计划评估在 2 岁随访时完成了 76 名患有科酮病的儿童和 82 名无科酮病的儿童,在 4 岁随访时完成了 55 名患有科酮病的儿童和 33 名无科酮病的儿童。患有科酮病的男孩在 KABC-II 学习(p=0·0424)和精神处理指数(MPI;p=0·0111)评估方面的表现比没有科酮病的男孩差,而女孩则没有。这些在男孩中观察到的差异可能是由发育迟缓引起的。在 4 岁随访时,患有或不患有科酮病的男孩和女孩之间的 KABC-II MPI 评分差异不显著。与没有科酮病的儿童相比,患有科酮病的男孩和女孩在两次随访时 BOT-2 精细运动技能(p<0·0001)和 KABC-II MPI 表现(2 岁:患有科酮病的男孩 p<0·0001,没有科酮病的男孩 p=0·0213;4 岁:患有科酮病的男孩 p=0·0256,没有科酮病的男孩 p=0·10)的得分较低。这些差异在男孩中并没有随着时间的推移而减弱,而女孩的分数则保持稳定,无论科酮病的状况如何。对于男孩,尿硫氰酸盐浓度的增加与 BOT-2 运动能力的降低显著相关(p=0·0321),但在女孩中并不显著相关,尿硫氰酸盐浓度与男孩或女孩的 KABC-II MPI 评分均无相关性。
与没有科酮病的男孩相比,患有科酮病的男孩在 2 岁随访时的运动和认知表现仍显著受损。由于这些损伤部分与尿液中硫氰酸盐测量的食用未加工木薯有关,因此迫切需要采取干预措施,以确保木薯加工得到改善,以去除这种食物来源的毒素。
美国国立卫生研究院。