Yuan Chen, Bao Ying, Sato Kaori, Nimptsch Katharina, Song Mingyang, Brand-Miller Jennie C, Morales-Oyarvide Vicente, Zoltick Emilie S, Keum NaNa, Wolpin Brian M, Meyerhardt Jeffrey A, Chan Andrew T, Willett Walter C, Stampfer Meir J, Wu Kana, Giovannucci Edward L, Fuchs Charles S, Ng Kimmie
Department of Medical Oncology, Dana-Farber Cancer Institute and Harvard Medical School, 450 Brookline Avenue, Boston, MA 02215, USA.
Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, MA, USA.
Br J Cancer. 2017 Sep 26;117(7):1079-1087. doi: 10.1038/bjc.2017.272. Epub 2017 Aug 17.
Although hyperinsulinemia is hypothesised to be involved in colorectal carcinogenesis, it remains unclear whether a diet inducing an elevated insulin response influences colorectal cancer (CRC) survival.
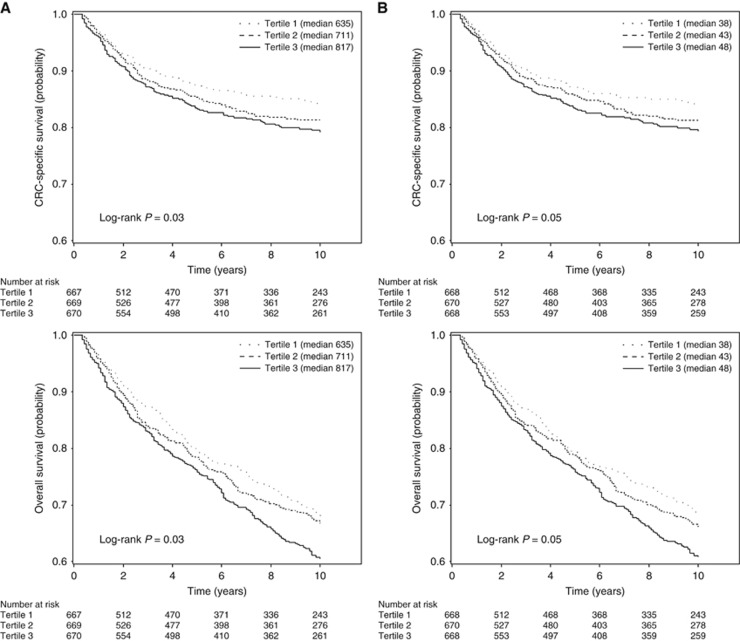
We examined the association of post-diagnosis dietary insulin scores with survival among 2006 patients from two large prospective cohorts who were diagnosed with CRC from 1976 to 2010. Dietary insulin load was calculated as a function of the food insulin index. Dietary insulin index was calculated by dividing insulin load by total energy intake. Cox proportional hazards models were used to calculate hazard ratios (HRs) for CRC-specific mortality and overall mortality, adjusted for other risk factors for cancer survival.
The adjusted HRs for CRC-specific mortality comparing the highest to the lowest quintiles were 1.82 (95% CI: 1.20-2.75, P=0.006) for dietary insulin load and 1.66 (95% CI: 1.10-2.50, P=0.004) for dietary insulin index. We also observed an increased risk for overall mortality, with adjusted HRs of 1.33 (95% CI: 1.03-1.72, P=0.03) for dietary insulin load and 1.32 (95% CI: 1.02-1.71, P=0.02) for dietary insulin index, comparing extreme quintiles. The increase in CRC-specific mortality associated with higher dietary insulin scores was more apparent among patients with body mass index (BMI)⩾25 kg m than BMI<25 kg m (P=0.01).
Higher dietary insulin scores after CRC diagnosis were associated with a statistically significant increase in CRC-specific and overall mortality.
尽管有假说认为高胰岛素血症与结直肠癌发生有关,但饮食诱导的胰岛素反应升高是否会影响结直肠癌(CRC)患者的生存仍不清楚。
我们在2006例于1976年至2010年期间被诊断为CRC的患者中,研究了诊断后饮食胰岛素评分与生存之间的关联,这些患者来自两个大型前瞻性队列。饮食胰岛素负荷根据食物胰岛素指数计算得出。饮食胰岛素指数通过将胰岛素负荷除以总能量摄入来计算。采用Cox比例风险模型计算结直肠癌特异性死亡率和总死亡率的风险比(HR),并对癌症生存的其他风险因素进行校正。
将最高五分位数与最低五分位数相比,饮食胰岛素负荷的结直肠癌特异性死亡率校正后HR为1.82(95%CI:1.20 - 2.75,P = 0.006),饮食胰岛素指数的校正后HR为1.66(95%CI:1.10 - 2.50,P = 0.004)。我们还观察到总死亡率风险增加,将极端五分位数相比,饮食胰岛素负荷的校正后HR为1.33(95%CI:1.03 - 1.72,P = 0.03),饮食胰岛素指数的校正后HR为1.32(95%CI:1.02 - 1.71,P = 0.02)。在体重指数(BMI)≥25 kg/m²的患者中,饮食胰岛素评分较高与结直肠癌特异性死亡率增加的关联比BMI < 25 kg/m²的患者更明显(P = 0.01)。
CRC诊断后较高的饮食胰岛素评分与结直肠癌特异性死亡率和总死亡率在统计学上显著增加相关。