Bukowski Radek, Hansen Nellie I, Pinar Halit, Willinger Marian, Reddy Uma M, Parker Corette B, Silver Robert M, Dudley Donald J, Stoll Barbara J, Saade George R, Koch Matthew A, Hogue Carol, Varner Michael W, Conway Deborah L, Coustan Donald, Goldenberg Robert L
The University of Texas at Austin Dell Medical School, Austin, Texas, United States of America.
RTI International, Research Triangle Park, North Carolina, United States of America.
PLoS One. 2017 Aug 18;12(8):e0182874. doi: 10.1371/journal.pone.0182874. eCollection 2017.
Worldwide, stillbirth is one of the leading causes of death. Altered fetal growth and placental abnormalities are the strongest and most prevalent known risk factors for stillbirth. The aim of this study was to identify patterns of association between placental abnormalities, fetal growth, and stillbirth.
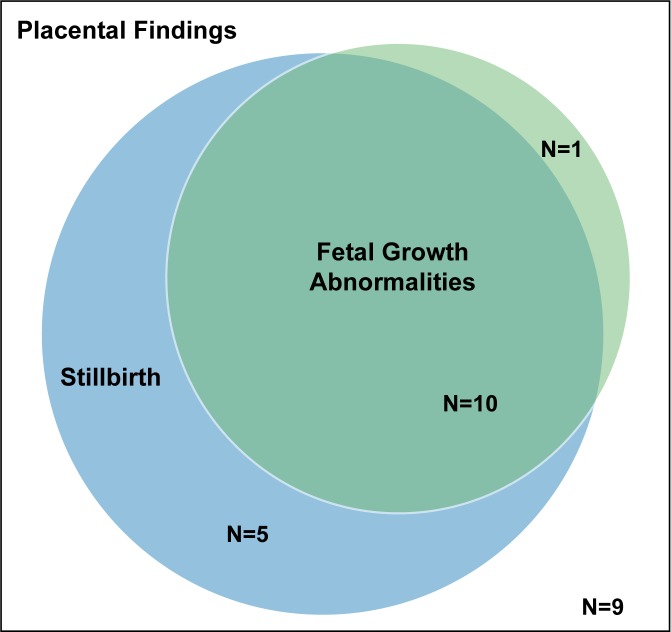
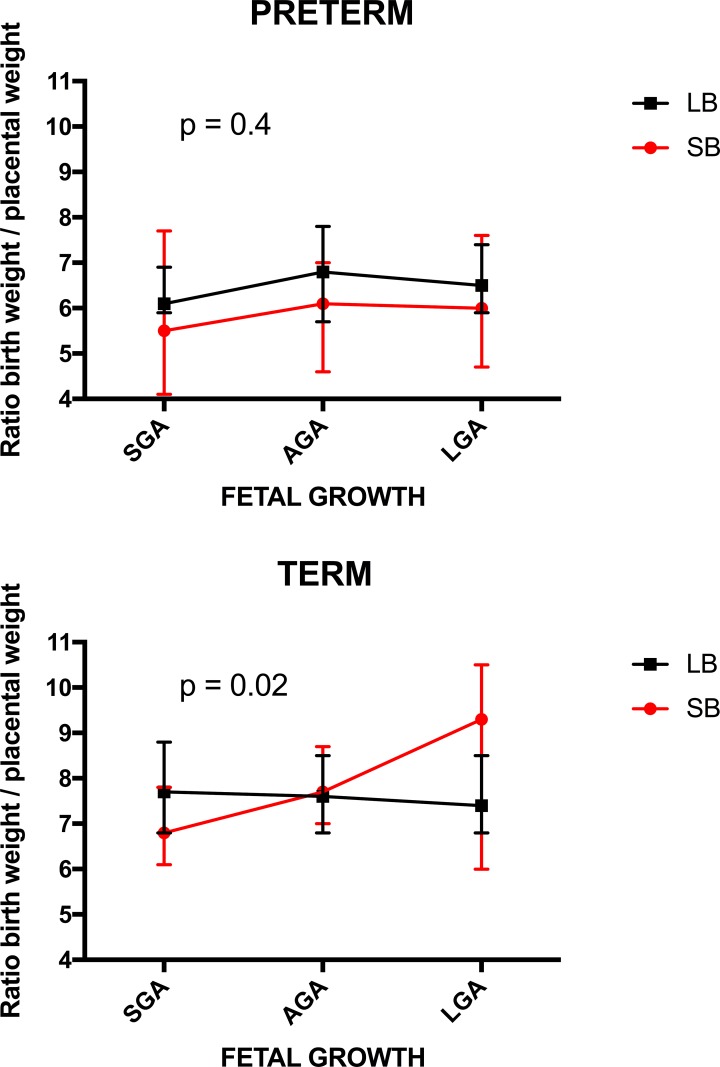
Population-based case-control study of all stillbirths and a representative sample of live births in 59 hospitals in 5 geographic areas in the U.S. Fetal growth abnormalities were categorized as small (<10th percentile) and large (>90th percentile) for gestational age at death (stillbirth) or delivery (live birth) using a published algorithm. Placental examination by perinatal pathologists was performed using a standardized protocol. Data were weighted to account for the sampling design. Among 319 singleton stillbirths and 1119 singleton live births at ≥24 weeks at death or delivery respectively, 25 placental findings were investigated. Fifteen findings were significantly associated with stillbirth. Ten of the 15 were also associated with fetal growth abnormalities (single umbilical artery; velamentous insertion; terminal villous immaturity; retroplacental hematoma; parenchymal infarction; intraparenchymal thrombus; avascular villi; placental edema; placental weight; ratio birth weight/placental weight) while 5 of the 15 associated with stillbirth were not associated with fetal growth abnormalities (acute chorioamnionitis of placental membranes; acute chorioamionitis of chorionic plate; chorionic plate vascular degenerative changes; perivillous, intervillous fibrin, fibrinoid deposition; fetal vascular thrombi in the chorionic plate). Five patterns were observed: placental findings associated with (1) stillbirth but not fetal growth abnormalities; (2) fetal growth abnormalities in stillbirths only; (3) fetal growth abnormalities in live births only; (4) fetal growth abnormalities in stillbirths and live births in a similar manner; (5) a different pattern of fetal growth abnormalities in stillbirths and live births.
The patterns of association between placental abnormalities, fetal growth, and stillbirth provide insights into the mechanism of impaired placental function and stillbirth. They also suggest implications for clinical care, especially for placental findings amenable to prenatal diagnosis using ultrasound that may be associated with term stillbirths.
在全球范围内,死产是主要死因之一。胎儿生长改变和胎盘异常是已知的导致死产的最强且最普遍的风险因素。本研究的目的是确定胎盘异常、胎儿生长与死产之间的关联模式。
对美国5个地理区域59家医院的所有死产病例及活产病例的代表性样本进行基于人群的病例对照研究。根据已发表的算法,将胎儿生长异常分为小于胎龄(<第10百分位数)和大于胎龄(>第90百分位数),分别针对死亡(死产)或分娩(活产)时的孕周。围产期病理学家采用标准化方案对胎盘进行检查。对数据进行加权以考虑抽样设计。在分别于死亡或分娩时孕周≥24周的319例单胎死产和1119例单胎活产中,对25项胎盘检查结果进行了调查。15项结果与死产显著相关。其中10项也与胎儿生长异常相关(单脐动脉;帆状附着;终末绒毛不成熟;胎盘后血肿;实质梗死;实质内血栓;无血管绒毛;胎盘水肿;胎盘重量;出生体重/胎盘重量比值),而与死产相关的15项结果中有5项与胎儿生长异常无关(胎盘膜急性绒毛膜羊膜炎;绒毛膜板急性绒毛膜羊膜炎;绒毛膜板血管退行性改变;绒毛周围、绒毛间隙纤维蛋白、类纤维蛋白沉积;绒毛膜板胎儿血管血栓)。观察到五种模式:胎盘检查结果与(1)死产相关但与胎儿生长异常无关;(2)仅与死产中的胎儿生长异常相关;(3)仅与活产中的胎儿生长异常相关;(4)以相似方式与死产和活产中的胎儿生长异常相关;(5)死产和活产中的胎儿生长异常模式不同。
胎盘异常、胎儿生长与死产之间的关联模式为胎盘功能受损和死产的机制提供了见解。它们还提示了对临床护理的意义,特别是对于可通过超声进行产前诊断且可能与足月死产相关的胎盘检查结果。