Sui Wilson, Lim Emerson A, Joel Decastro G, McKiernan James M, Anderson Christopher B
Department of Urology, Columbia University Medical Center, New York, NY, USA.
Department of Medicine, Columbia University Medical Center, New York, NY, USA.
Bladder Cancer. 2017 Jul 27;3(3):181-189. doi: 10.3233/BLC-170107.
To compare the outcomes of adjuvant chemotherapy (AC) versus observation in patients with non-organ confined disease after neoadjuvant chemotherapy and radical cystectomy (RC).
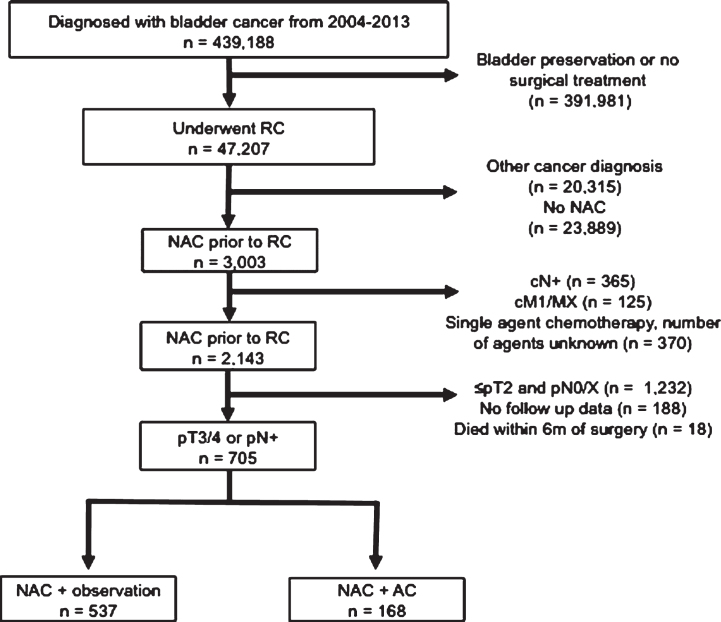
Using the National Cancer Database, we identified patients who received NAC prior to RC and had advanced stage (pT3/4) or pathologically involved nodes (pN+) at the time of surgery from 2004-2013. We determined whether patients then received AC or were managed with observation only and used multivariable proportional hazards regression to estimate the impact of AC on overall survival.
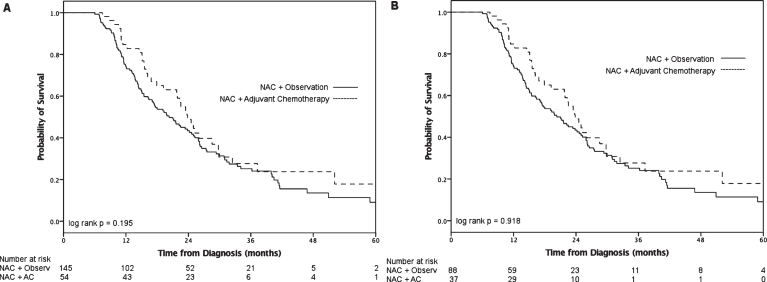
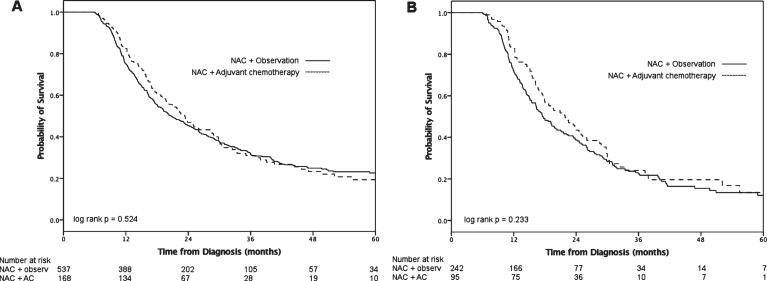
Overall 34% (N = 705) of patients who received NAC and underwent RC were pT3/4 and/or pN+. Of these patients, 24% (N = 168) received subsequent chemotherapy and the rest were observed. Median survival for the entire cohort was 21 months (IQR 12-45). There was not a statistically significant difference in median survival between the AC and observation groups (23 months [IQR 14-46] versus 20 months [IQR 12-46], log-rank = 0.52). On multivariate analysis there was no survival advantage for the AC cohort. Subgroup analysis of pN+ patients who received AC also did not show a survival advantage.
Patients who are pT3/4 and/or pN+ after NAC and RC have a poor prognosis. The addition of AC does not seem to be beneficial. Further research should focus identifying patients who may benefit from additional chemotherapy.
比较新辅助化疗及根治性膀胱切除术后非器官局限性疾病患者接受辅助化疗(AC)与观察等待的疗效。
利用国家癌症数据库,我们确定了2004年至2013年期间在根治性膀胱切除术(RC)前接受新辅助化疗(NAC)且手术时处于晚期(pT3/4)或病理检查发现淋巴结受累(pN+)的患者。我们确定这些患者随后是否接受了AC治疗或仅接受观察等待,并使用多变量比例风险回归来评估AC对总生存期的影响。
总体而言,接受NAC并接受RC的患者中有34%(N = 705)为pT3/4和/或pN+。在这些患者中,24%(N = 168)接受了后续化疗,其余患者接受观察等待。整个队列的中位生存期为21个月(四分位间距12 - 45)。AC组和观察等待组的中位生存期无统计学显著差异(23个月[四分位间距14 - 46]对20个月[四分位间距12 - 46],对数秩检验=0.52)。多变量分析显示AC组没有生存优势。对接受AC治疗的pN+患者进行亚组分析也未显示出生存优势。
新辅助化疗及根治性膀胱切除术后pT3/4和/或pN+的患者预后较差。加用AC似乎并无益处。进一步的研究应聚焦于确定可能从额外化疗中获益的患者。