Davies Benjamin M, Patel Hiren C
Department of Neurosurgery, Greater Manchester Neuroscience Centre, Salford Royal Foundation Trust (SRFT), Salford, United Kingdom.
Surg J (N Y). 2016 Aug 10;2(3):e70-e77. doi: 10.1055/s-0036-1587691. eCollection 2016 Jul.
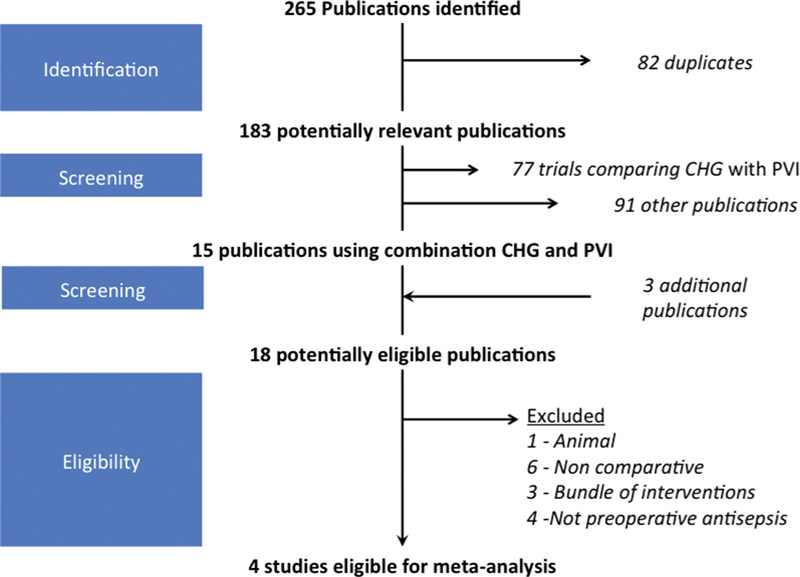
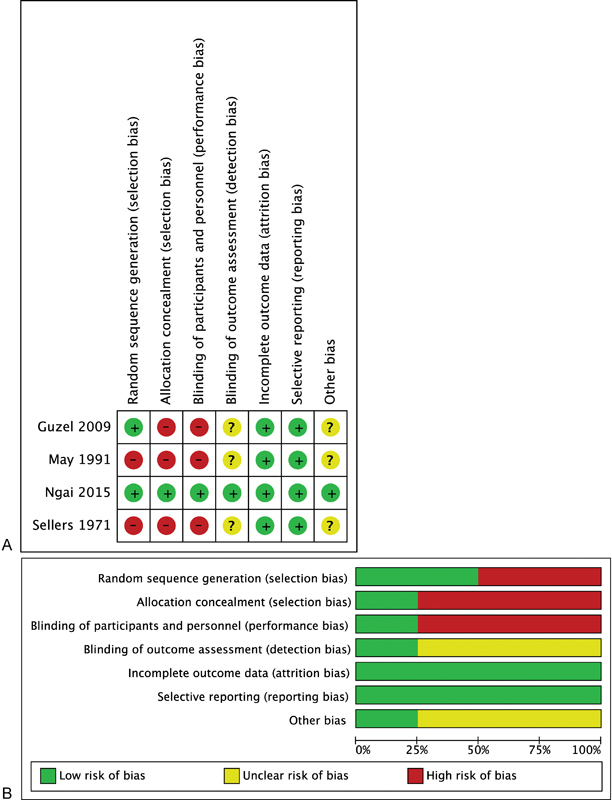
Effective preoperative antisepsis is recognized to prevent surgical site infection (SSI), although the definitive method is unclear. Many have compared chlorhexidine (CHG) with povidone-iodine (PVI), but there is emerging evidence for combination usage. To conduct a systematic review and meta-analysis to evaluate if combination skin preparation (1) reduces colonization at the operative site and (2) prevents SSI compared with single-agent use. A literature search of MEDLINE, Embase, and Cochrane Database of Clinical Trials was performed. Comparative, human trials considering the combination use of CHG and PVI, as preoperative antisepsis, to single-agent CHG or PVI use were included. Studies were excluded from meta-analysis if the use or absence of alcohol was inconsistent between study arms. The study was performed using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The primary outcome for meta-analysis was surgical site infection. The secondary outcome was colonization at the operative site. Eighteen publications with a combination of CHG and PVI use were identified. Of these, 12/14 inferred promise for combination usage, including four trials eligible for meta-analysis. Only one trial reported SSI as its outcome. The remaining three considered bacterial colonization. Combination preparation had a pooled odds ratio for complete decolonization of 5.62 (95% confidence interval 3.2 to 9.7, < 0.00001). There was no evidence of heterogeneity (Cochran's Q 2.1, 2 , = 0.35). There is emerging, albeit low-quality, evidence in favor of combination CHG and PVI preoperative antisepsis. Further rigorous investigation is indicated.
有效的术前抗菌措施被认为可预防手术部位感染(SSI),尽管确切方法尚不清楚。许多人已将氯己定(CHG)与聚维酮碘(PVI)进行了比较,但越来越多的证据支持联合使用。 进行系统评价和荟萃分析,以评估联合皮肤准备(1)与单药使用相比是否能减少手术部位的定植,以及(2)预防手术部位感染。 对MEDLINE、Embase和Cochrane临床试验数据库进行了文献检索。 纳入了将CHG和PVI联合使用作为术前抗菌措施与单药CHG或PVI使用进行比较的人体试验。如果研究组之间酒精的使用或未使用情况不一致,则将研究排除在荟萃分析之外。 使用PRISMA(系统评价和荟萃分析首选报告项目)指南进行研究。 荟萃分析的主要结局是手术部位感染。次要结局是手术部位的定植。 共识别出18篇关于CHG和PVI联合使用的出版物。其中,12/14推断联合使用有前景,包括四项符合荟萃分析条件的试验。只有一项试验将手术部位感染作为其结局。其余三项考虑的是细菌定植。联合制剂完全去定植的合并比值比为5.62(95%置信区间3.2至9.7, <0.00001)。没有异质性证据(Cochrane's Q 2.1,2 , =0.35)。 有新出现的、尽管质量较低的证据支持CHG和PVI联合术前抗菌。需要进一步进行严格的调查。