Service de Transplantation Rénale, Hôpital Necker, Université Paris Descartes, Paris, France; INSERM UMRS_1163, IHU Imagine, Paris, France.
Columbia Center for Translational Immunology, Department of Medicine, Columbia University, New York, NY 10032, USA; Department of Surgery, Columbia University, New York, NY 10032, USA; Department of Microbiology and Immunology, Columbia University Center, New York, NY 10032, USA.
Trends Immunol. 2017 Nov;38(11):829-843. doi: 10.1016/j.it.2017.07.008. Epub 2017 Aug 18.
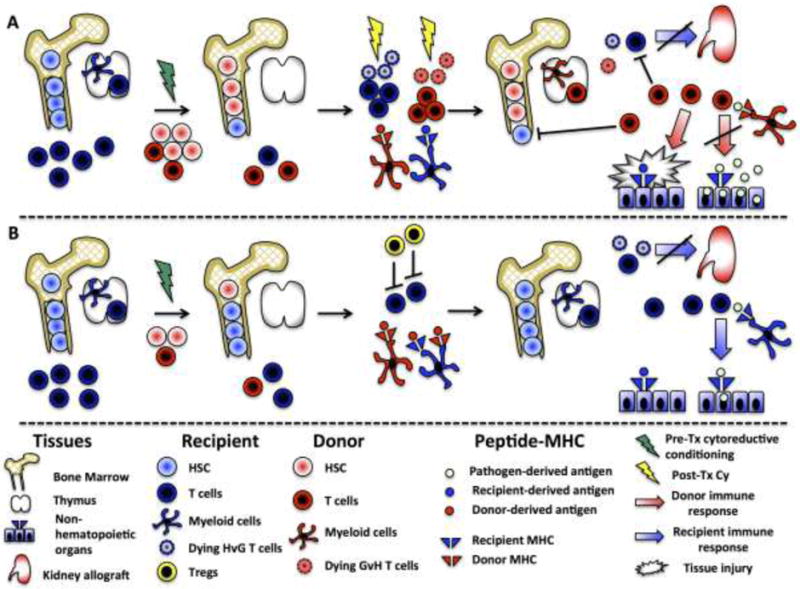
Immune responses to allografts represent a major barrier in organ transplantation. Immune tolerance to avoid chronic immunosuppression is a critical goal in the field, recently achieved in the clinic by combining bone marrow transplantation (BMT) with kidney transplantation following non-myeloablative conditioning. At high levels of chimerism such protocols can permit central deletional tolerance, but with a significant risk of graft-versus-host (GVH) disease (GVHD). By contrast, transient chimerism-based tolerance is devoid of GVHD risk and appears to initially depend on regulatory T cells (Tregs) followed by gradual, presumably peripheral, clonal deletion of donor-reactive T cells. Here we review recent mechanistic insights into tolerance and the development of more robust and safer protocols for tolerance induction that will be guided by innovative immune monitoring tools.
同种异体移植物的免疫反应是器官移植中的一个主要障碍。避免慢性免疫抑制的免疫耐受是该领域的一个关键目标,最近通过骨髓移植 (BMT) 与非清髓性预处理后的肾移植相结合在临床上实现了这一目标。在高水平嵌合的情况下,这些方案可以允许中枢性删除性耐受,但存在显著的移植物抗宿主病 (GVHD) 风险。相比之下,短暂的嵌合耐受没有 GVHD 风险,并且似乎最初依赖于调节性 T 细胞 (Tregs),随后是供体反应性 T 细胞的逐渐、可能是外周的克隆删除。在这里,我们综述了最近关于耐受的机制见解,以及开发更强大和更安全的耐受诱导方案的进展,这些方案将受到创新免疫监测工具的指导。