Chan Yap-Hang, Hai Jo Jo, Lau Kui-Kai, Li Sheung-Wai, Lau Chu-Pak, Siu Chung-Wah, Yiu Kai-Hang, Tse Hung-Fat
Division of Cardiology, Department of Medicine, Queen Mary Hospital, University of Hong Kong, Rm 1928, Block K, Hong Kong, China.
Division of Neurology, University of Hong Kong, Hong Kong, China.
BMC Cardiovasc Disord. 2017 Aug 24;17(1):233. doi: 10.1186/s12872-017-0667-2.
Whether PR prolongation independently predicts new-onset ischemic events of myocardial infarction and stroke was unclear. Underlying pathophysiological mechanisms of PR prolongation leading to adverse cardiovascular events were poorly understood. We investigated the role of PR prolongation in pathophysiologically-related adverse cardiovascular events and underlying mechanisms.
We prospectively investigated 597 high-risk cardiovascular outpatients (mean age 66 ± 11 yrs.; male 67%; coronary disease 55%, stroke 22%, diabetes 52%) for new-onset ischemic stroke, myocardial infarction (MI), congestive heart failure (CHF), and cardiovascular death. Vascular phenotype was determined by carotid intima-media thickness (IMT).
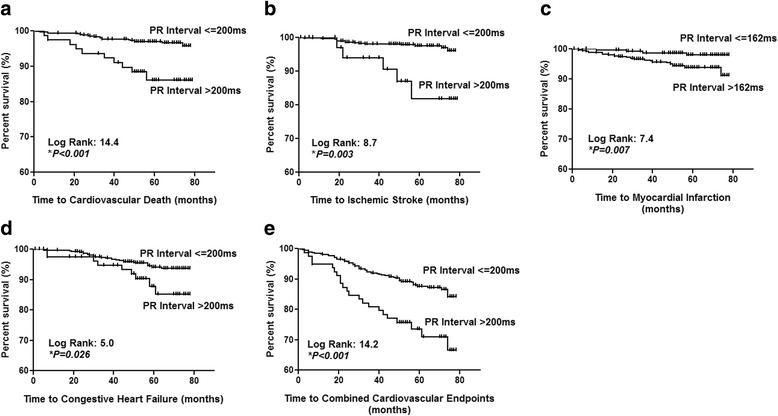
PR prolongation >200 ms was present in 79 patients (13%) at baseline. PR prolongation >200 ms was associated with significantly higher mean carotid IMT (1.05 ± 0.37 mm vs 0.94 ± 0.28 mm, P = 0.010). After mean study period of 63 ± 11 months, increased PR interval significantly predicted new-onset ischemic stroke (P = 0.006), CHF (P = 0.040), cardiovascular death (P < 0.001), and combined cardiovascular endpoints (P < 0.001) at cut-off >200 ms. Using multivariable Cox regression, PR prolongation >200 ms independently predicted new-onset ischemic stroke (HR 8.6, 95% CI: 1.9-37.8, P = 0.005), cardiovascular death (HR 14.1, 95% CI: 3.8-51.4, P < 0.001) and combined cardiovascular endpoints (HR 2.4, 95% CI: 1.30-4.43, P = 0.005). PR interval predicts new-onset MI at the exploratory cut-off >162 ms (C-statistic 0.70, P = 0.001; HR: 8.0, 95% CI: 1.65-38.85, P = 0.010).
PR prolongation strongly predicts new-onset ischemic stroke, MI, cardiovascular death, and combined cardiovascular endpoint including CHF in coronary patients or risk equivalent. Adverse vascular function may implicate an intermediate pathophysiological phenotype or mediating mechanism.
PR间期延长是否能独立预测心肌梗死和中风等新发缺血性事件尚不清楚。导致不良心血管事件的PR间期延长的潜在病理生理机制了解甚少。我们研究了PR间期延长在病理生理相关不良心血管事件中的作用及其潜在机制。
我们前瞻性地调查了597例高危心血管门诊患者(平均年龄66±11岁;男性占67%;冠心病占55%,中风占22%,糖尿病占52%),观察新发缺血性中风、心肌梗死(MI)、充血性心力衰竭(CHF)和心血管死亡情况。通过颈动脉内膜中层厚度(IMT)确定血管表型。
基线时79例患者(13%)PR间期延长>200毫秒。PR间期延长>200毫秒与平均颈动脉IMT显著升高相关(1.05±0.37毫米对0.94±0.28毫米,P=0.010)。平均研究期63±11个月后,PR间期延长在截断值>200毫秒时显著预测新发缺血性中风(P=0.006)、CHF(P=0.040)、心血管死亡(P<0.001)以及综合心血管终点事件(P<0.001)。使用多变量Cox回归分析,PR间期延长>200毫秒独立预测新发缺血性中风(风险比8.6,95%置信区间:1.9-37.8,P=0.005)、心血管死亡(风险比14.1,95%置信区间:3.8-51.4,P<0.001)以及综合心血管终点事件(风险比2.4,95%置信区间:1.30-4.43,P=0.005)。PR间期在探索性截断值>162毫秒时预测新发MI(C统计量0.70,P=0.001;风险比:8.0,95%置信区间:1.65-38.85,P=0.010)。
PR间期延长强烈预测冠心病患者或风险相当者的新发缺血性中风、MI、心血管死亡以及包括CHF在内的综合心血管终点事件。不良血管功能可能涉及一种中间病理生理表型或介导机制。