Department of Surgery, Buddhist Tzu Chi General Hospital, Hualien, Taiwan.
Department of Colorectal Surgery, Buddhist Tzu Chi General Hospital, 707, Section 3, Chung Yang Road, Hualien, 970, Taiwan.
World J Surg Oncol. 2017 Aug 25;15(1):164. doi: 10.1186/s12957-017-1228-y.
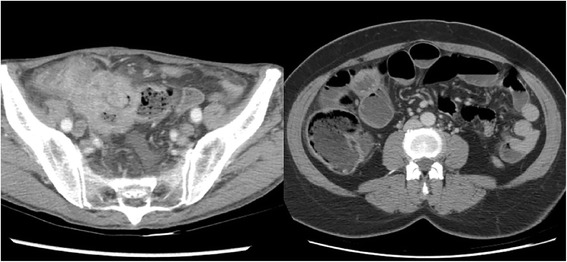
Emergency complications of colon cancer include perforation and obstruction which were recognized as poor prognostic factors. Few studies have directly compared the outcomes of these two groups. In this study, we evaluated mortality and morbidity in patients with colon cancer initially presenting as perforation and obstruction.
Newly diagnosed colon cancer cases initially presenting with perforation or obstruction at Tzu Chi General Hospital, Hualien, Taiwan, between 2009 and 2015 were included. Cases of iatrogenic perforation or perforation sites far away from the tumor sites and rectal (< 15 cm from the anal verge) cancer were excluded. Progression-free survival, local recurrence rate, distant metastasis rate, and overall survival were the evaluated outcomes.
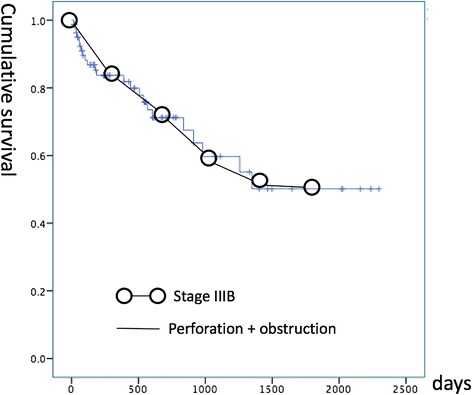
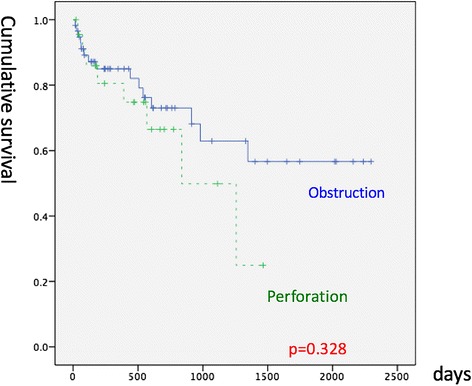
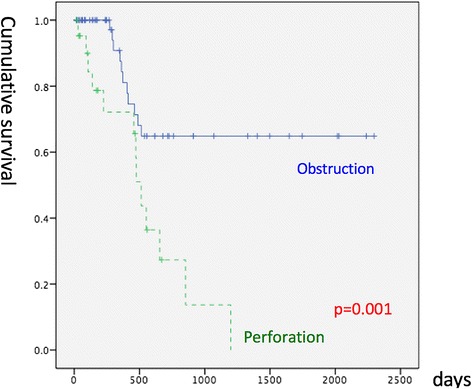
Eighty-one patients met the selection criteria; 23 and 58 patients had perforation and obstruction, respectively, as the initial symptom. The median age was 72 years. The median tumor stage was stage IIIB. The 1-year and 3-year survival rates were 83.7 and 59.7%, respectively. The perforation group (PRG) and obstruction group (OBG) did not differ significantly in intensive care unit (ICU) stay rate (p = 0.147), sex (p = 0.45), comorbidities (heart, liver, and renal diseases and diabetes mellitus), median stage (p = 0.198), and overall survival (p = 0.328). However, PRG had a higher age at diagnosis (74 vs. 64 years, p = 0.037), a higher APACHE II score (12 vs. 7, p = 0.002), lower disease-free survival (p = 0.001), a higher recurrence rate (56.5 vs. 19%, p = 0.002), a higher distant metastasis rate (39.1 vs. 13.8%, p = 0.015), and a higher local recurrence rate (43.5 vs. 5.2%, p < 0.001) than did OBG. OBG had a higher two-stage operation rate (46.6 vs. 17.4%, p = 0.022). After adjustment for the tumor stage, comorbidity (chronic renal disease), body mass index (BMI), and adjuvant chemotherapy or radiotherapy in multivariate statistics, PRG had lower disease-free survival (p = 0.005) than OBG but overall survival was identical.
For colon cancer initially presenting as perforation or obstruction, the PRG had poorer progression-free survival, a higher local recurrence rate, and a higher distant metastasis rate than did OBG. Overall survival did not differ between these two groups.
结肠癌的紧急并发症包括穿孔和梗阻,这些并发症被认为是预后不良的因素。很少有研究直接比较这两组患者的结局。在本研究中,我们评估了以穿孔和梗阻为首发症状的结肠癌患者的死亡率和发病率。
2009 年至 2015 年,在花莲慈济医院诊断为结肠癌且最初表现为穿孔或梗阻的新病例被纳入研究。医源性穿孔或穿孔部位远离肿瘤部位以及直肠(<肛门缘 15cm)癌的病例被排除在外。无进展生存期、局部复发率、远处转移率和总生存期是评估的结果。
81 例患者符合入选标准;23 例和 58 例患者的首发症状分别为穿孔和梗阻。中位年龄为 72 岁。中位肿瘤分期为 IIIB 期。1 年和 3 年生存率分别为 83.7%和 59.7%。穿孔组(PRG)和梗阻组(OBG)在 ICU 入住率(p=0.147)、性别(p=0.45)、合并症(心脏病、肝病、肾病和糖尿病)、中位分期(p=0.198)和总生存率(p=0.328)方面无显著差异。然而,PRG 的诊断年龄更高(74 岁 vs. 64 岁,p=0.037)、APACHE II 评分更高(12 分 vs. 7 分,p=0.002)、无疾病生存率更低(p=0.001)、复发率更高(56.5% vs. 19%,p=0.002)、远处转移率更高(39.1% vs. 13.8%,p=0.015)和局部复发率更高(43.5% vs. 5.2%,p<0.001)。OBG 的两阶段手术率更高(46.6% vs. 17.4%,p=0.022)。在多变量统计中,调整肿瘤分期、合并症(慢性肾脏病)、体重指数(BMI)和辅助化疗或放疗后,PRG 的无疾病生存率(p=0.005)低于 OBG,但总生存率相同。
对于以穿孔或梗阻为首发表现的结肠癌,PRG 的无进展生存期更差,局部复发率和远处转移率更高,而总生存率无差异。