Division of Intensive Care, Department of Anesthesiology and Intensive Care Medicine, Jichi Medical University School of Medicine, 3311-1, Yakushiji, Shimotsuke, Tochigi, 329-0498, Japan.
Crit Care. 2017 Aug 25;21(1):229. doi: 10.1186/s13054-017-1815-x.
Endothelial activation and damage occur early during sepsis, with activated coagulopathy and playing a major role in the pathophysiology of sepsis-induced acute kidney injury (AKI). The aim of this study was to compare the various biomarkers of endothelial injury with the biomarkers of coagulation and inflammation and to determine a significant predictor of AKI in patients with sepsis.
We conducted a single-center, retrospective, observational study on patients with sepsis fulfilling the Third International Consensus Definitions for Sepsis and Septic Shock criteria admitted to an adult intensive care unit (ICU) at a university hospital from June 2011 to December 2016. Levels of 13 biomarkers were measured on ICU admission, including markers of endothelial injury (soluble thrombomodulin [sTM], E-selectin, protein C, and plasminogen activator inhibitor-1 [PAI-1]) and markers of coagulation derangement (platelet count, fibrin degradation product [FDP], prothrombin time [PT], fibrinogen, α-plasminogen inhibitor [α-PI], antithrombin III [AT III], plasminogen, thrombin-antithrombin complex, and plasmin-α-plasmin inhibitor complex). All patients with sepsis were reviewed, and the development of AKI was evaluated. Multivariate logistic regression analysis was performed to identify significant independent predictive factors for AKI.
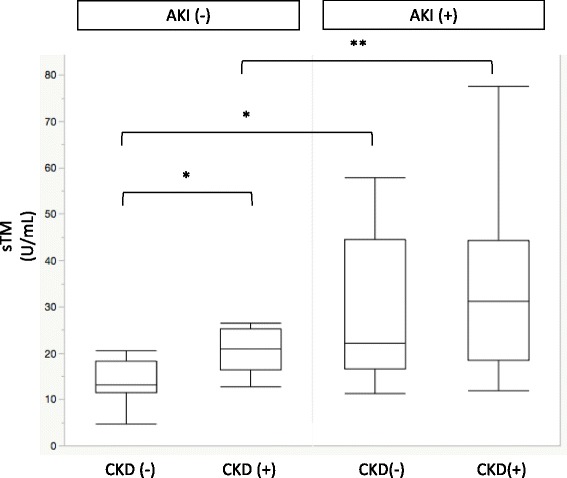
Of the 514 patients admitted with sepsis, 351 (68.3%) developed AKI. Compared with the non-AKI group, all the endothelial biomarkers were significantly different in the AKI group (sTM [23.6 vs. 15.6 U/ml, P < 0.0001], E-selectin [65.5 vs. 46.2 ng/ml, P = 0.0497], PAI-1 [180.4 vs. 75.3 ng/ml, P = 0.018], and protein C [45.9 vs. 58.7 ng/ml, P < 0.0001]). Biomarkers of coagulopathy and inflammation, platelet counts, FDP, PT, α-PI, AT III, plasminogen, and C-reactive protein were significantly different between the two groups. Multivariable logistic regression analysis showed that sTM was an independent predictive factor of AKI, with an AUROC of 0.758 (P < 0.0001).
Endothelial biomarkers were significantly changed in the sepsis patients with AKI. Particularly, sTM was an independent predictive biomarker for the development of AKI that outperformed other coagulation and inflammation biomarkers as well as organ function in patients with sepsis.
内皮细胞激活和损伤发生在脓毒症早期,同时伴有激活的凝血异常,并在脓毒症引起的急性肾损伤(AKI)的病理生理学中起主要作用。本研究的目的是比较内皮损伤的各种生物标志物与凝血和炎症的生物标志物,并确定脓毒症患者 AKI 的显著预测因子。
我们对 2011 年 6 月至 2016 年 12 月在一所大学医院成人重症监护病房(ICU)收治的符合第三次国际脓毒症和脓毒性休克定义共识标准的脓毒症患者进行了一项单中心、回顾性、观察性研究。在 ICU 入院时测量了 13 种生物标志物的水平,包括内皮损伤标志物(可溶性血栓调节蛋白[sTM]、E-选择素、蛋白 C 和纤溶酶原激活物抑制剂-1[PAI-1])和凝血失调标志物(血小板计数、纤维蛋白降解产物[FDP]、凝血酶原时间[PT]、纤维蛋白原、α- 纤溶酶原抑制剂[α-PI]、抗凝血酶 III[AT III]、纤溶酶原、凝血酶-抗凝血酶复合物和纤溶酶-α- 纤溶酶抑制剂复合物)。对所有脓毒症患者进行了回顾性分析,并评估了 AKI 的发生情况。进行了多变量逻辑回归分析,以确定 AKI 的显著独立预测因素。
在 514 例因脓毒症入院的患者中,351 例(68.3%)发生 AKI。与非 AKI 组相比,AKI 组的所有内皮生物标志物均有显著差异(sTM [23.6 与 15.6 U/ml,P < 0.0001]、E-选择素 [65.5 与 46.2 ng/ml,P = 0.0497]、PAI-1 [180.4 与 75.3 ng/ml,P = 0.018]和蛋白 C [45.9 与 58.7 ng/ml,P < 0.0001])。凝血和炎症标志物、血小板计数、FDP、PT、α-PI、AT III、纤溶酶原和 C 反应蛋白在两组之间也有显著差异。多变量逻辑回归分析显示,sTM 是 AKI 的独立预测因子,AUROC 为 0.758(P < 0.0001)。
脓毒症合并 AKI 患者的内皮生物标志物发生明显变化。特别是 sTM 是 AKI 发展的独立预测生物标志物,其表现优于脓毒症患者的其他凝血和炎症标志物以及器官功能。