Department of Surgery, Chang Gung Memorial Hospital, Linkou, Taiwan, Republic of China.
2College of Medicine, Chang Gung University, Guishan, Taoyuan, Taiwan, Republic of China.
World J Emerg Surg. 2018 Sep 10;13:41. doi: 10.1186/s13017-018-0202-5. eCollection 2018.
Sepsis is a syndrome characterized by a constellation of clinical manifestations and a significantly high mortality rate in the surgical intensive care unit (ICU). It is frequently complicated by acute kidney injury (AKI), which, in turn, increases the risk of mortality. Therefore, it is of paramount importance to identify those septic patients at risk for the development of AKI and mortality. The objective of this pilot study was to evaluate several different biomarkers, including NGAL, calprotectin, KIM-1, cystatin C, and GDF-15, along with SOFA scores, in predicting the development of septic AKI and associated in-hospital mortality in critically ill surgical patients.
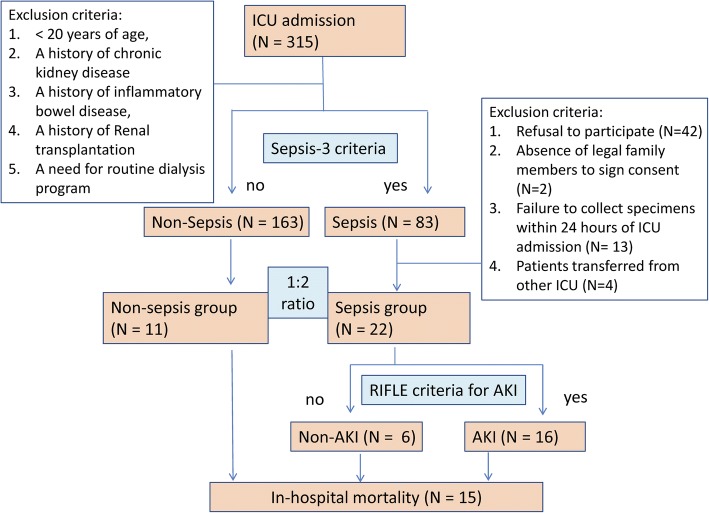
Patients admitted to the surgical ICU were prospectively enrolled, having given signed informed consent. Their blood and urine samples were obtained and subjected to enzyme-linked immunosorbent assay (ELISA) to determine the levels of various novel biomarkers. The clinical data and survival outcome were recorded and analyzed.
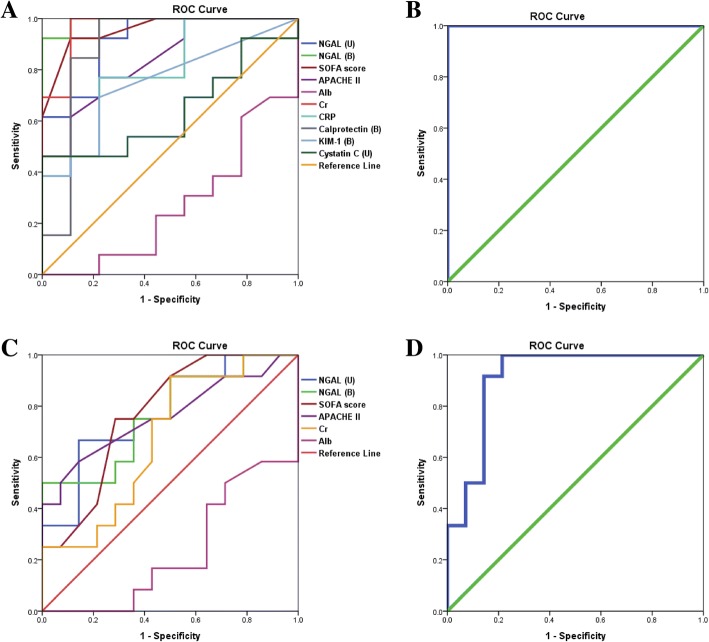
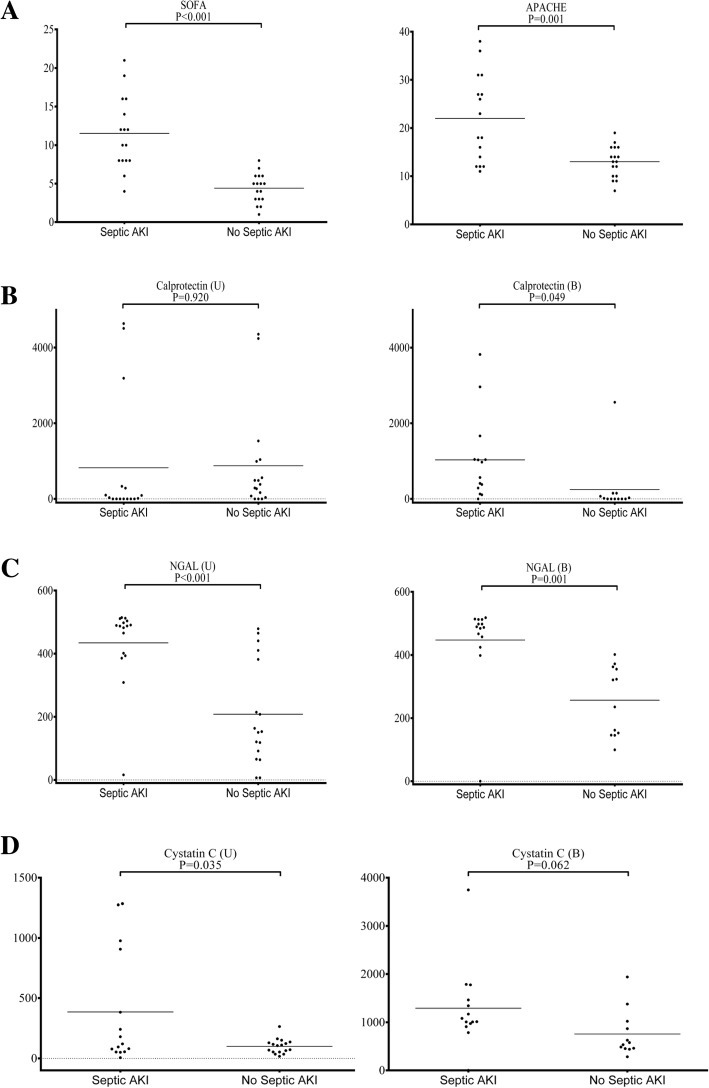
A total of 33 patients were enrolled in the study. Most patients received surgery prior to ICU admission, with abdominal surgery being the most common type of procedure (27 patients (81.8%)). In the study, 22 patients had a diagnosis of sepsis with varying degrees of AKI, while the remaining 11 were free of sepsis. Statistical analysis demonstrated that in patients with septic AKI versus those without, the following were significantly higher: serum NGAL (447.5 ± 35.7 ng/mL vs. 256.5 ± 31.8 ng/mL, value 0.001), calprotectin (1030.3 ± 298.6 pg/mL vs. 248.1 ± 210.7 pg/mL, value 0.049), urinary NGAL (434.2 ± 31.5 ng/mL vs. 208.3 ± 39.5 ng/mL, value < 0.001), and SOFA score (11.5 ± 1.2 vs. 4.4 ± 0.5, value < 0.001). On the other hand, serum NGAL (428.2 ± 32.3 ng/mL vs. 300.4 ± 44.3 ng/mL, value 0.029) and urinary NGAL (422.3 ± 33.7 ng/mL vs. 230.8 ± 42.2 ng/mL, value 0.001), together with SOFA scores (10.6 ± 1.4 vs. 5.6 ± 0.8, value 0.003), were statistically higher in cases of in-hospital mortality. A combination of serum NGAL, urinary NGAL, and SOFA scores could predict in-hospital mortality with an AUROC of 0.911.
This pilot study demonstrated a promising panel that allows an early diagnosis, high sensitivity, and specificity and a prognostic value for septic AKI and in-hospital mortality in surgical ICU. Further study is warranted to validate our findings.
脓毒症是一种以一系列临床表现为特征的综合征,在外科重症监护病房(ICU)的死亡率非常高。它常伴有急性肾损伤(AKI),这反过来又增加了死亡率。因此,识别那些有发生 AKI 和死亡风险的脓毒症患者至关重要。本初步研究的目的是评估几种不同的生物标志物,包括 NGAL、钙卫蛋白、KIM-1、胱抑素 C 和 GDF-15,以及 SOFA 评分,以预测危重症外科患者发生脓毒症 AKI 及相关院内死亡的风险。
前瞻性纳入入住外科 ICU 的患者,并获得其签署的知情同意书。采集他们的血液和尿液样本,并进行酶联免疫吸附试验(ELISA)以确定各种新型生物标志物的水平。记录并分析临床数据和生存结果。
共有 33 名患者入组本研究。大多数患者在入住 ICU 前接受了手术,其中腹部手术最为常见(27 例(81.8%))。在本研究中,22 例患者被诊断为脓毒症,其 AKI 程度不一,而其余 11 例患者无脓毒症。统计分析表明,与无脓毒症 AKI 的患者相比,脓毒症 AKI 患者的以下指标显著更高:血清 NGAL(447.5±35.7ng/mL 比 256.5±31.8ng/mL, 值 0.001)、钙卫蛋白(1030.3±298.6pg/mL 比 248.1±210.7pg/mL, 值 0.049)、尿 NGAL(434.2±31.5ng/mL 比 208.3±39.5ng/mL, 值<0.001)和 SOFA 评分(11.5±1.2 比 4.4±0.5, 值<0.001)。另一方面,血清 NGAL(428.2±32.3ng/mL 比 300.4±44.3ng/mL, 值 0.029)和尿 NGAL(422.3±33.7ng/mL 比 230.8±42.2ng/mL, 值 0.001)以及 SOFA 评分(10.6±1.4 比 5.6±0.8, 值 0.003)在院内死亡病例中均更高。血清 NGAL、尿 NGAL 和 SOFA 评分的联合可预测院内死亡率,其 AUROC 为 0.911。
本初步研究显示了一个有前途的组合,可早期诊断、高灵敏度、特异性,并对外科 ICU 中的脓毒症 AKI 和院内死亡具有预后价值。需要进一步的研究来验证我们的发现。