Bouchard Josée, Malhotra Rakesh, Shah Shamik, Kao Yu-Ting, Vaida Florin, Gupta Akanksha, Berg David T, Grinnell Brian W, Stofan Brenda, Tolwani Ashita J, Mehta Ravindra L
Division of Nephrology and Hypertension, Department of Medicine, University of California San Diego, San Diego, California, United States of America; Division of Nephrology, Department of Medicine, Université de Montréal, Montréal, Canada.
Division of Nephrology and Hypertension, Department of Medicine, University of California San Diego, San Diego, California, United States of America.
PLoS One. 2015 Mar 19;10(3):e0120770. doi: 10.1371/journal.pone.0120770. eCollection 2015.
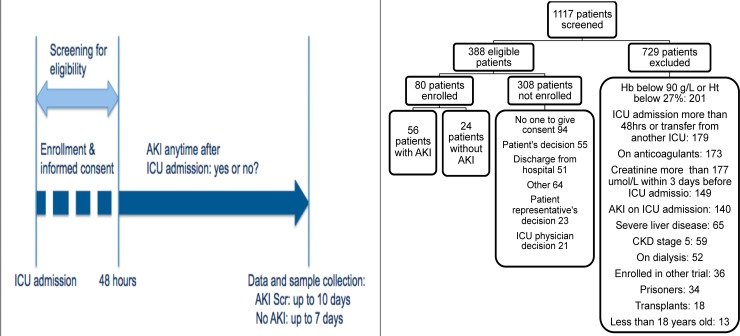
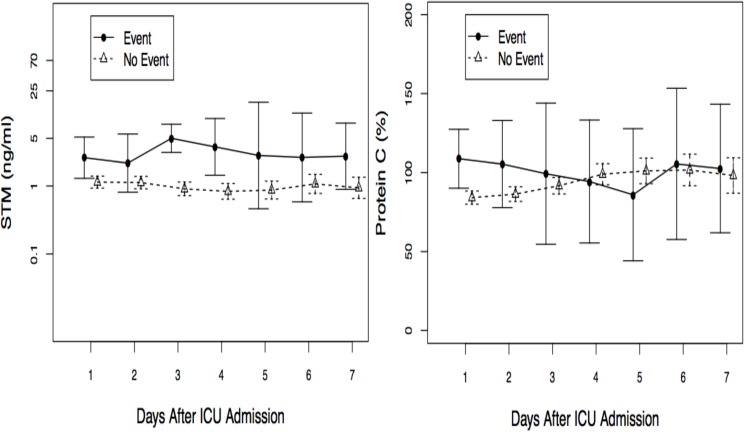
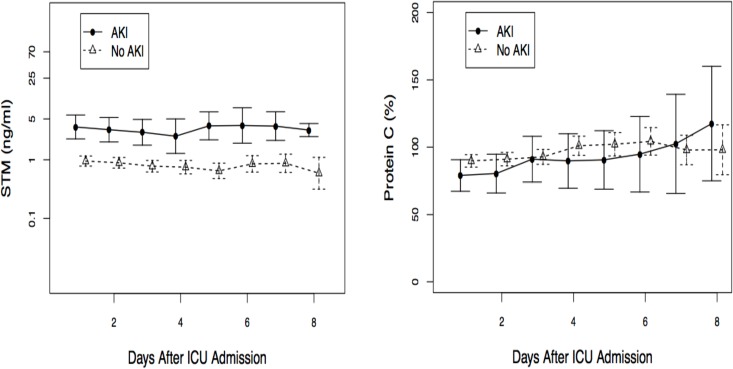
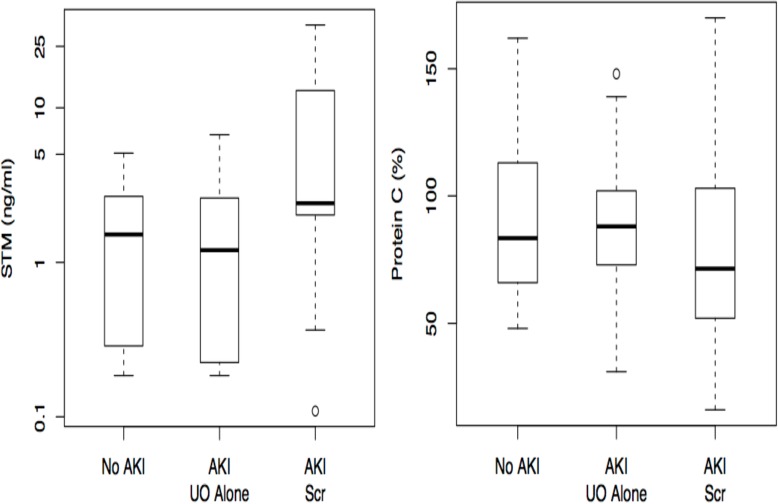
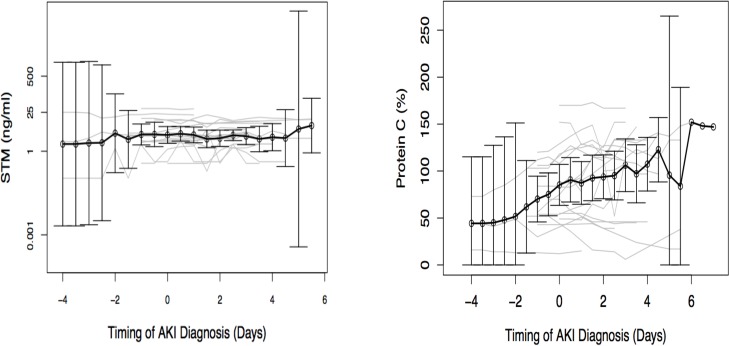
Endothelial dysfunction contributes to the development of acute kidney injury (AKI) in animal models of ischemia reperfusion injury and sepsis. There are limited data on markers of endothelial dysfunction in human AKI. We hypothesized that Protein C (PC) and soluble thrombomodulin (sTM) levels could predict AKI. We conducted a multicenter prospective study in 80 patients to assess the relationship of PC and sTM levels to AKI, defined by the AKIN creatinine (AKI Scr) and urine output criteria (AKI UO). We measured marker levels for up to 10 days from intensive care unit admission. We used area under the curve (AUC) and time-dependent multivariable Cox proportional hazard model to predict AKI and logistic regression to predict mortality/non-renal recovery. Protein C and sTM were not different in patients with AKI UO only versus no AKI. On intensive care unit admission, as PC levels are usually lower with AKI Scr, the AUC to predict the absence of AKI was 0.63 (95%CI 0.44-0.78). The AUC using log10 sTM levels to predict AKI was 0.77 (95%CI 0.62-0.89), which predicted AKI Scr better than serum and urine neutrophil gelatinase-associated lipocalin (NGAL) and cystatin C, urine kidney injury molecule-1 and liver-fatty acid-binding protein. In multivariable models, PC and urine NGAL levels independently predicted AKI (p=0.04 and 0.02) and PC levels independently predicted mortality/non-renal recovery (p=0.04). In our study, PC and sTM levels can predict AKI Scr but are not modified during AKI UO alone. PC levels could independently predict mortality/non-renal recovery. Additional larger studies are needed to define the relationship between markers of endothelial dysfunction and AKI.
在内皮功能障碍有助于缺血再灌注损伤和脓毒症动物模型中急性肾损伤(AKI)的发展。关于人类急性肾损伤中内皮功能障碍标志物的数据有限。我们假设蛋白C(PC)和可溶性血栓调节蛋白(sTM)水平可以预测急性肾损伤。我们对80名患者进行了一项多中心前瞻性研究,以评估PC和sTM水平与急性肾损伤的关系,急性肾损伤由急性肾损伤网络(AKIN)肌酐(AKI Scr)和尿量标准(AKI UO)定义。我们从重症监护病房入院起最多10天测量标志物水平。我们使用曲线下面积(AUC)和时间依赖性多变量Cox比例风险模型来预测急性肾损伤,并使用逻辑回归来预测死亡率/非肾恢复情况。仅符合AKI UO标准的患者与无急性肾损伤的患者相比,PC和sTM没有差异。在重症监护病房入院时,由于急性肾损伤患者的PC水平通常较低,预测无急性肾损伤的AUC为0.63(95%CI 0.44 - 0.78)。使用log10 sTM水平预测急性肾损伤的AUC为0.77(95%CI 0.62 - 0.89),其预测急性肾损伤肌酐比血清和尿液中性粒细胞明胶酶相关脂质运载蛋白(NGAL)、胱抑素C、尿肾损伤分子-1和肝脂肪酸结合蛋白更好。在多变量模型中,PC和尿液NGAL水平独立预测急性肾损伤(p = 0.04和0.02),PC水平独立预测死亡率/非肾恢复情况(p = 0.04)。在我们的研究中,PC和sTM水平可以预测急性肾损伤肌酐,但仅在急性肾损伤尿量标准时无变化。PC水平可以独立预测死亡率/非肾恢复情况。需要更多大型研究来确定内皮功能障碍标志物与急性肾损伤之间的关系。