Madaline Theresa, Nori Priya, Mowrey Wenzhu, Zukowski Elisabeth, Gohil Shruti, Sarwar Uzma, Weston Gregory, Urrely Riganni, Palombelli Matthew, Pierino Vinnie Frank, Parsons Vanessa, Ehrlich Amy, Ostrowsky Belinda, Corpuz Marilou, Pirofski Liise-Anne
Division of Infectious Diseases, Department of Medicine.
Division of Biostatistics, Department of Epidemiology and Population Health and.
Open Forum Infect Dis. 2017 Jun 29;4(2):ofx097. doi: 10.1093/ofid/ofx097. eCollection 2017 Spring.
A streamlined transition from inpatient to outpatient care can decrease 30-day readmissions. Outpatient parenteral antibiotic therapy (OPAT) programs have not reduced readmissions; an OPAT bundle has been suggested to improve outcomes. We implemented a transition-of-care (TOC) OPAT bundle and assessed the effects on all-cause, 30-day hospital readmission.
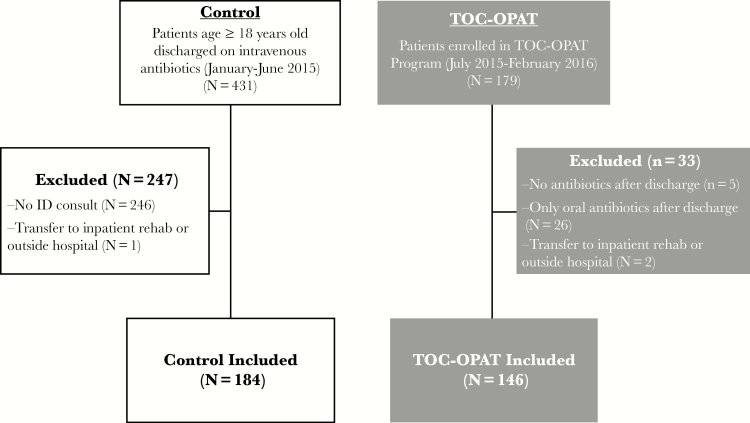
Retrospectively, patients receiving postdischarge intravenous antibiotics were evaluated before and after implementation of a TOC-OPAT program in Bronx, New York, between July, 2015 and February, 2016. Pearson's χ test was used to compare 30-day readmissions between groups, and logistic regression was used to adjust for covariates. Time from discharge to readmission was analyzed to assess readmission risk, using log-rank test to compare survival curves and Cox proportional hazards model to adjust for covariates. Secondary outcomes, 30-day emergency department (ED) visits, and mortality were analyzed similarly.
Compared with previous standard care (n = 184), the TOC-OPAT group (n = 146) had significantly lower 30-day readmissions before (13.0% vs 26.1%, < .01) and after adjustment for covariates (odds ratio [OR] = 0.51; 95% confidence interval [CI], 0.27-0.94; = .03). In time-dependent analyses, TOC-OPAT patients were at significantly lower risk for readmission (log-rank test, < .01; hazard ratio = 0.56; 95% CI, 0.32-0.97; = .04). Propensity-matched sensitivity analysis showed lower readmissions in the TOC-OPAT group (13.6% vs 24.6%, = .04), which was attenuated after adjustment (OR = 0.51; 95% CI, 0.25-1.05; = .07). Mortality and ED visits were similar in both groups.
Our TOC-OPAT patients had reduced 30-day readmissions compared with the previous standard of care. An effective TOC-OPAT bundle can successfully improve patient outcomes in an economically disadvantaged area.
从住院治疗到门诊治疗的简化过渡可降低30天再入院率。门诊胃肠外抗生素治疗(OPAT)项目并未降低再入院率;有人建议采用OPAT综合方案来改善治疗效果。我们实施了一项护理过渡(TOC)OPAT综合方案,并评估了其对全因30天医院再入院率的影响。
回顾性地评估了2015年7月至2016年2月在纽约布朗克斯实施TOC-OPAT项目前后接受出院后静脉用抗生素治疗的患者。采用Pearson卡方检验比较两组间的30天再入院率,并采用逻辑回归分析对协变量进行校正。分析从出院到再入院的时间以评估再入院风险,采用对数秩检验比较生存曲线,并采用Cox比例风险模型对协变量进行校正。对次要结局、30天急诊科就诊情况和死亡率进行了类似分析。
与先前的标准治疗组(n = 184)相比,TOC-OPAT组(n = 146)在调整协变量之前(13.0%对26.1%,P <.01)和之后(比值比[OR]=0.51;95%置信区间[CI],0.27 - 0.94;P =.03)的30天再入院率均显著降低。在时间依赖性分析中,TOC-OPAT患者的再入院风险显著降低(对数秩检验,P <.01;风险比 = 0.56;95% CI,0.32 - 0.97;P =.04)。倾向匹配敏感性分析显示TOC-OPAT组的再入院率较低(13.6%对24.6%,P =.04),调整后该差异有所减弱(OR = 0.51;95% CI,0.25 - 1.05;P =.07)。两组的死亡率和急诊科就诊情况相似。
与先前的标准治疗相比,我们的TOC-OPAT患者30天再入院率降低。有效的TOC-OPAT综合方案可在经济条件不利地区成功改善患者治疗效果。