Division of Clinical Oncology, Department of Internal Medicine, Medical University of Graz, Auenbruggerplatz 15, 8036, Graz, Austria.
Research Unit Genetic Epidemiology and Pharmacogenetics, Medical University of Graz, Graz, Austria.
Clin Transl Oncol. 2017 Nov;19(11):1400-1408. doi: 10.1007/s12094-017-1742-y. Epub 2017 Aug 29.
The cure rate of stage I seminoma patients is close to 100% and so the recent focus of clinical research has shifted onto the prevention of treatment-related complications. We assessed long-term cardiovascular complications and identified risk factors for cardiovascular events (CVEs) in stage I seminoma patients.
This retrospective cohort study included 406 consecutive stage I seminoma patients. Primary endpoint was CVE rate.
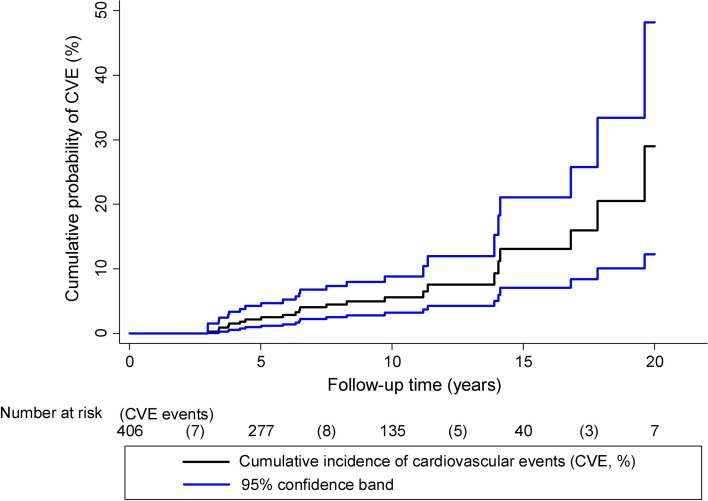
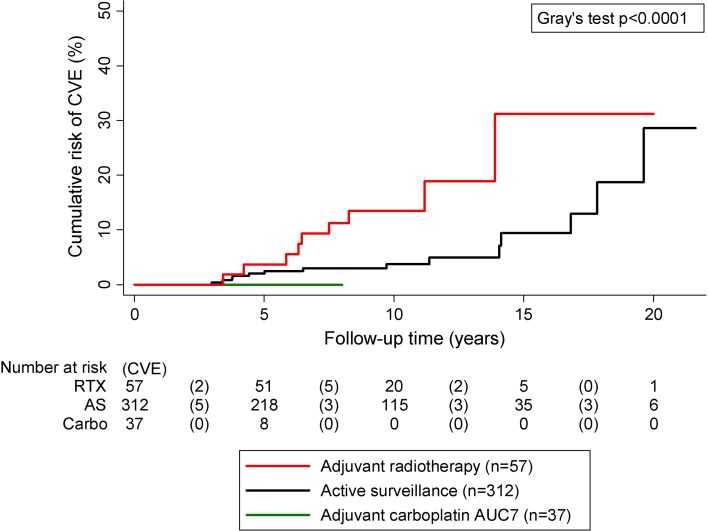
During a median follow-up of 8.6 years, we observed 23 CVEs in 406 patients [10-year CVE risk 5.6% (95% CI 3.2 to 8.8)]. In univariable competing risk analysis, higher age, positive smoking status, history of diabetes and hypertension were significantly associated with the occurrence of CVE. In multi-state analysis, new onset of diabetes, hypertension and hyperlipidemia during follow-up predicted for an excessively increased CVE risk. In multivariable analysis adjusting for age and smoking, the development of hypertension and hyperlipidemia after tumor-specific treatment prevailed as risk factors for CVE. Regarding adjuvant treatment modalities, patients receiving adjuvant radiotherapy had a significantly higher probability of CVE than patients receiving adjuvant carboplatin [16% vs. 0%; risk difference (RD) = 16%, 95% CI 6 to 25%, p = 0.001]. This difference prevailed after adjusting for age, follow-up-time, diabetes, hypertension and smoking (RD = 11%, 95% CI 1 to 20%, p = 0.025).
We identified a panel of baseline risk factors and dynamically, occurring predictors of CVE in stage I seminoma patients. This information may be used for targeting comorbidity management in these patients. The observed association of adjuvant radiotherapy with higher CVE risk warrants further investigation.
I 期精原细胞瘤患者的治愈率接近 100%,因此,临床研究的重点已转移到预防治疗相关并发症上。我们评估了长期心血管并发症,并确定了 I 期精原细胞瘤患者心血管事件(CVE)的风险因素。
这是一项回顾性队列研究,共纳入 406 例连续的 I 期精原细胞瘤患者。主要终点是 CVE 发生率。
在中位随访 8.6 年期间,我们在 406 例患者中观察到 23 例 CVE[10 年 CVE 风险为 5.6%(95%CI 3.2 至 8.8)]。在单变量竞争风险分析中,较高的年龄、阳性吸烟状态、糖尿病和高血压病史与 CVE 的发生显著相关。在多状态分析中,随访期间新发糖尿病、高血压和高脂血症预测 CVE 风险过高。在调整年龄和吸烟因素的多变量分析中,肿瘤特异性治疗后高血压和高脂血症的发展成为 CVE 的危险因素。关于辅助治疗方式,接受辅助放疗的患者发生 CVE 的概率明显高于接受辅助卡铂治疗的患者[16%比 0%;风险差异(RD)=16%,95%CI 6%至 25%,p=0.001]。在调整年龄、随访时间、糖尿病、高血压和吸烟因素后,这种差异仍然存在(RD=11%,95%CI 1%至 20%,p=0.025)。
我们确定了一组与 I 期精原细胞瘤患者 CVE 相关的基线风险因素和动态发生的预测因素。这些信息可用于这些患者的合并症管理。观察到辅助放疗与更高的 CVE 风险相关,值得进一步研究。