Shi Yu, Xiong Jiachuan, Chen Yan, Deng Junna, Peng Hongmei, Zhao Jinghong, He Jing
Institute of Nephrology of Chongqing and Kidney Center of PLA, Xinqiao Hospital, Third Military Medical University, Chongqing, China.
Int Urol Nephrol. 2018 Feb;50(2):301-312. doi: 10.1007/s11255-017-1679-7. Epub 2017 Aug 30.
To assess the efficacy of the multidisciplinary care (MDC) model for patients with chronic kidney disease (CKD).
The MDC model has been used in clinical practice for years, but the effectiveness of the MDC model for patients with CKD remains controversial.
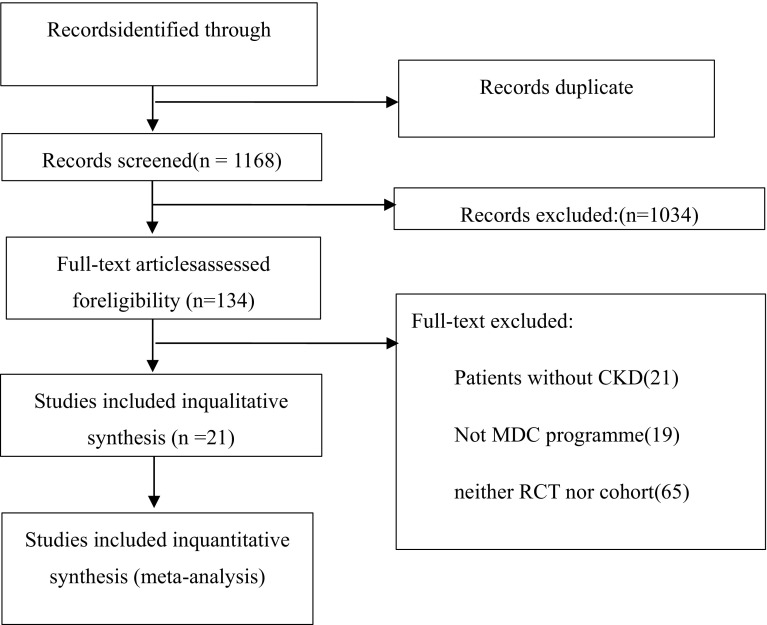
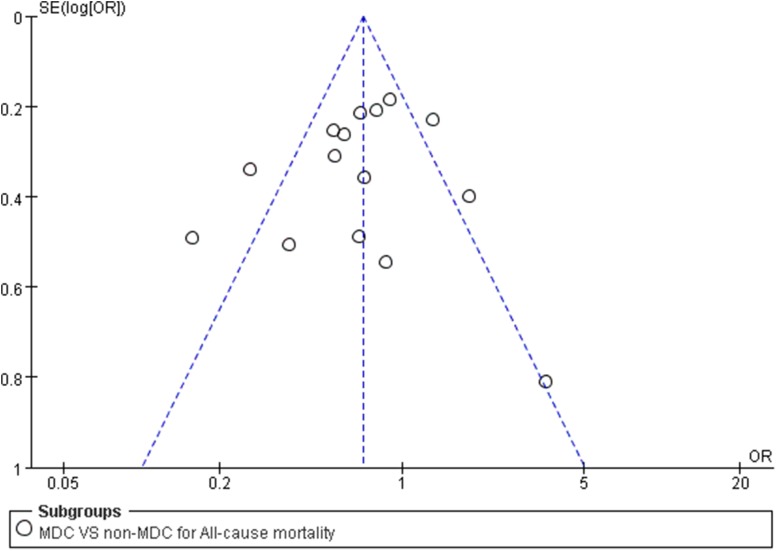
Embase, PubMed, Medline, the Cochrane Library, and China National Knowledge Infrastructure databases were used to search for relevant articles. Only randomized controlled trials and cohort studies were pooled. Two independent authors assessed all articles and extracted the data. The efficacy was estimated from the odds ratios and corresponding 95% confidence intervals. A random effects model was used according to the heterogeneity.
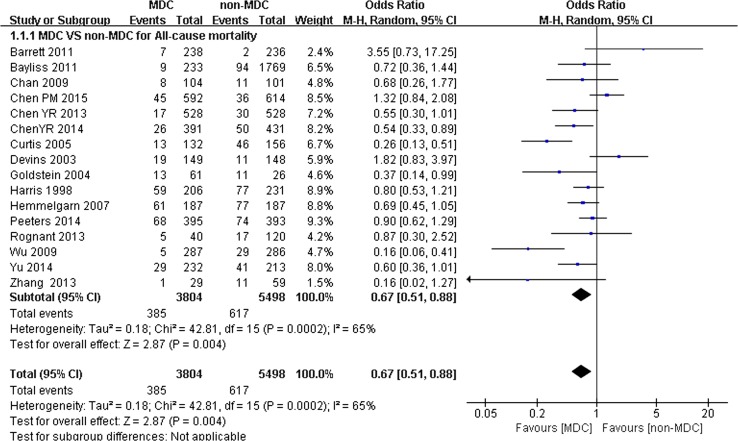
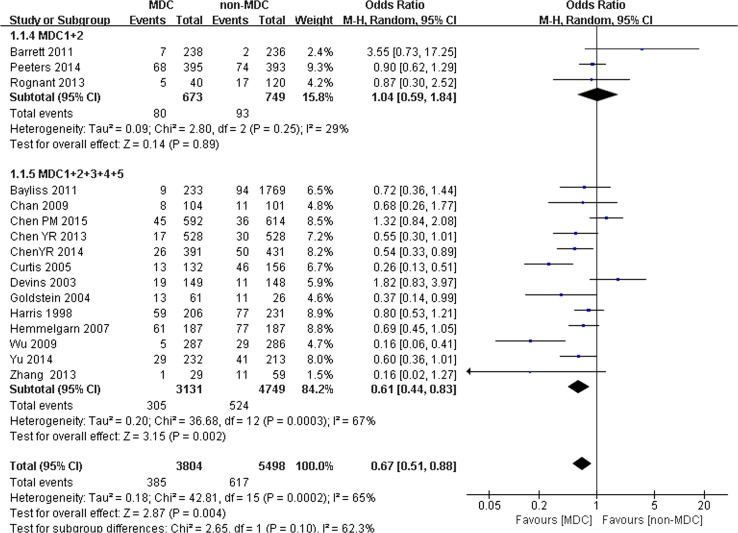
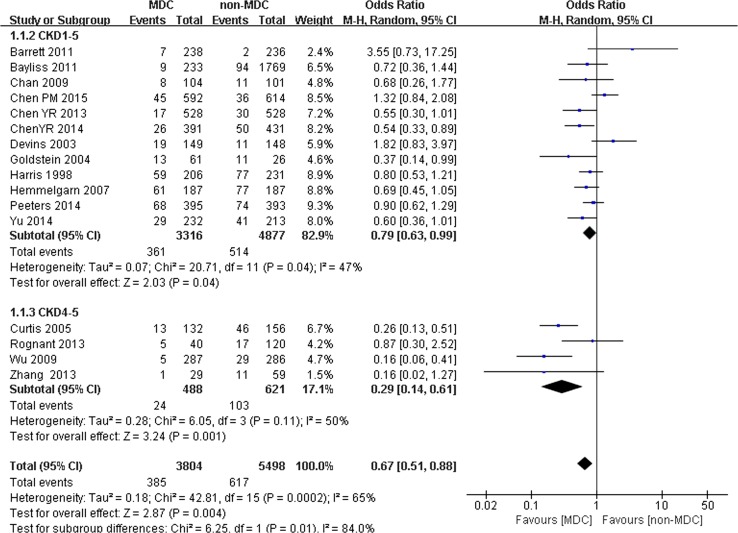
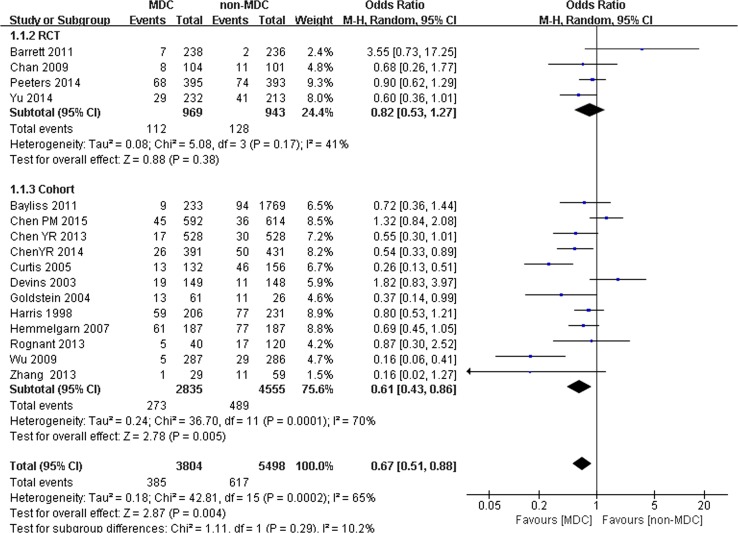
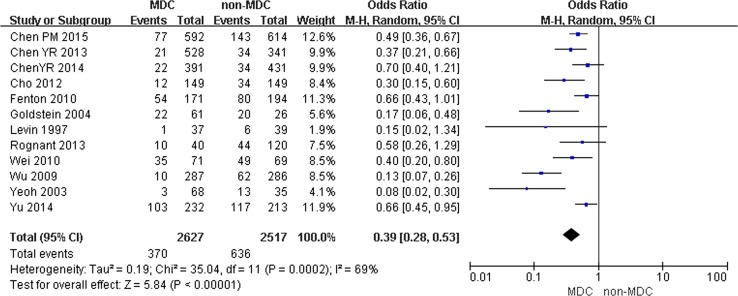
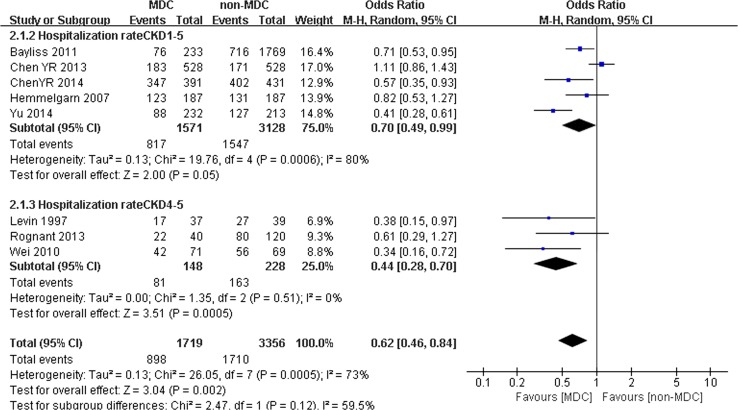
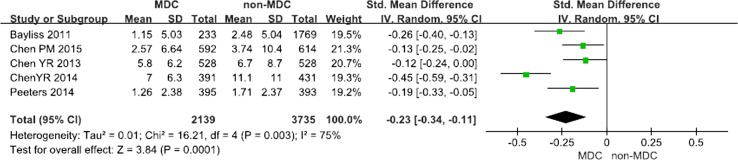
Twenty-one studies including 10,284 participants were analyzed. Compared with the non-MDC group, MDC was associated with a lower risk of all-cause mortality and lower hospitalization rates for patients with CKD. In addition, MDC also resulted in a slower eGFR decline and reduced temporary catheterization for patients receiving dialysis. However, according to the subgroup analysis, the lower rates of all-cause mortality in the MDC group were observed only in patients in stage 4-5 and when the staff of the MDC consisted of nephrologists, nurse specialists and professionals from other fields. The most prominent effect of reducing the hospitalization rates was also observed in patients with stage 4-5 but not in patients with stage 4-5 CKD.
MDC can lower the all-cause mortality of patients with CKD, reduce temporary catheterization for patients receiving dialysis, decrease the hospitalization rate, and slow the eGFR decline. Moreover, the reduction in all-cause mortality crucially depends on the professionals comprising the MDC staff and the stage of CKD in patients. In addition, the CKD stage influences the hospitalization rates.
评估多学科护理(MDC)模式对慢性肾脏病(CKD)患者的疗效。
MDC模式已在临床实践中应用多年,但该模式对CKD患者的有效性仍存在争议。
使用Embase、PubMed、Medline、Cochrane图书馆和中国知网数据库检索相关文章。仅汇总随机对照试验和队列研究。两位独立作者评估所有文章并提取数据。根据优势比和相应的95%置信区间估计疗效。根据异质性使用随机效应模型。
分析了21项研究,共10284名参与者。与非MDC组相比,MDC与CKD患者全因死亡率较低和住院率较低相关。此外,MDC还导致接受透析患者的估算肾小球滤过率(eGFR)下降较慢,并减少了临时导管插入术。然而,根据亚组分析,仅在4-5期患者以及MDC工作人员由肾病学家、专科护士和其他领域专业人员组成时,才观察到MDC组全因死亡率较低。降低住院率的最显著效果也在4-5期患者中观察到,但在4-5期CKD患者中未观察到。
MDC可降低CKD患者的全因死亡率,减少接受透析患者的临时导管插入术,降低住院率,并减缓eGFR下降。此外,全因死亡率的降低关键取决于组成MDC工作人员的专业人员以及患者的CKD阶段。此外,CKD阶段会影响住院率。