Ekerstad Niklas, Bylin Kristoffer, Karlson Björn W
Department of Cardiology, NU (NÄL-Uddevalla) Hospital Group, Trollhättan.
Department of Medical and Health Sciences, Division of Health Care Analysis, Linköping University, Linköping.
Drug Healthc Patient Saf. 2017 Aug 18;9:77-88. doi: 10.2147/DHPS.S139237. eCollection 2017.
Early readmissions of frail elderly patients after an episode of hospital care are common and constitute a crucial patient safety outcome. Our purpose was to study the impact of medications on such early rehospitalizations.
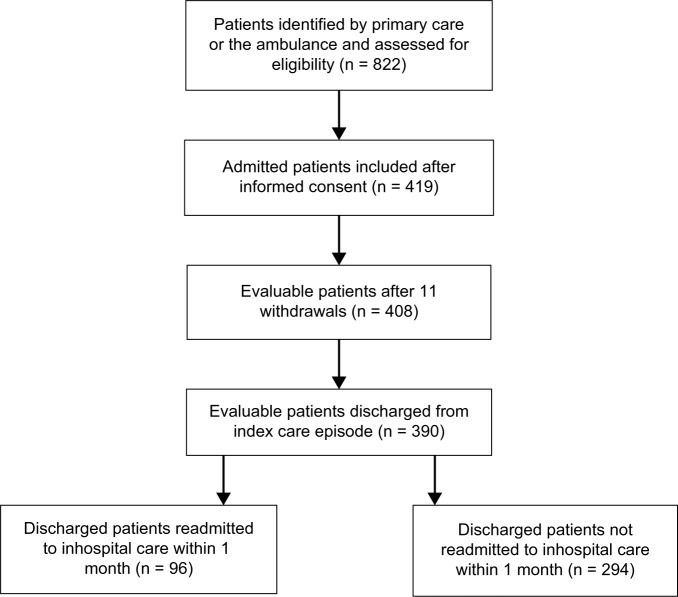
This is a clinical, prospective, observational study on rehospitalizations within 30 days after an acute hospital episode for frail patients over the age of 75 years. To identify adverse drug reactions (ADRs), underuse of evidence-based treatment and avoidability of rehospitalizations, the Naranjo score, the Hallas criteria and clinical judgment were used.
Of 390 evaluable patients, 96 (24.6%) were rehospitalized. The most frequent symptoms and conditions were dyspnea (n = 25) and worsened general condition (n = 18). The most frequent diagnoses were heart failure (n = 17) and pneumonia/acute bronchitis (n = 13). By logistic regression analysis, independent risk predictors for rehospitalization were heart failure (odds ratio [OR] = 1.8; 95% CI = 1.1-3.1) and anemia (OR = 2.3; 95% CI = 1.3-4.0). The number of rehospitalizations due to probable ADRs was 13, of which two were assessed as avoidable. The number of rehospitalizations probably due to underuse of evidence-based drug treatment was 19, all of which were assessed as avoidable. The number of rehospitalizations not due to ADRs or underuse of evidence-based drug treatment was 64, of which none was assessed as avoidable.
One out of four frail elderly patients discharged from hospital was rehospitalized within 1 month. Although ADRs constituted an important cause of rehospitalization, underuse of evidence-based drug treatment might be an even more frequent cause. Potentially avoidable rehospitalizations were more frequently associated with underuse of evidence-based drug treatment than with ADRs. Efforts to avoid ADRs in frail elderly patients must be balanced and combined with evidence-based drug therapy, which can benefit these patients.
体弱老年患者在住院治疗后早期再入院情况较为常见,是患者安全的一项关键结果。我们的目的是研究药物对这种早期再入院的影响。
这是一项针对75岁以上体弱患者急性住院后30天内再入院情况的临床、前瞻性观察性研究。为识别药物不良反应(ADR)、循证治疗的未充分使用情况以及再入院的可避免性,采用了纳朗霍评分、哈拉斯标准和临床判断。
在390例可评估患者中,96例(24.6%)再次入院。最常见的症状和病情是呼吸困难(n = 25)和一般状况恶化(n = 18)。最常见的诊断是心力衰竭(n = 17)和肺炎/急性支气管炎(n = 13)。通过逻辑回归分析,再入院的独立风险预测因素是心力衰竭(比值比[OR]=1.8;95%置信区间[CI]=1.1 - 3.1)和贫血(OR = 2.3;95% CI = 1.3 - 4.0)。因可能的ADR导致的再入院次数为13次,其中2次被评估为可避免。可能因循证药物治疗未充分使用导致的再入院次数为19次,所有这些均被评估为可避免。非因ADR或循证药物治疗未充分使用导致的再入院次数为64次,其中无一例被评估为可避免。
四分之一出院的体弱老年患者在1个月内再次入院。虽然ADR是再入院的一个重要原因,但循证药物治疗的未充分使用可能是更常见的原因。潜在可避免的再入院与循证药物治疗未充分使用的关联比与ADR更为频繁。在体弱老年患者中避免ADR的努力必须保持平衡,并与循证药物治疗相结合,这对这些患者有益。