Department of Biostatistics and Epidemiology, The Center for Clinical Epidemiology and Biostatistics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA.
Department of Family Medicine and Community Health, University of Pennsylvania, Philadelphia, PA, USA.
Arch Gerontol Geriatr. 2017 Nov;73:248-256. doi: 10.1016/j.archger.2017.08.005. Epub 2017 Aug 24.
The ability to predict mortality and admission to acute care hospitals, skilled nursing facilities (SNFs), and long-term care (LTC) facilities in the elderly and how it varies by activity of daily living (ADL) and instrumental ADL (IADL) status could be useful in measuring the success or failure of economic, social, or health policies aimed at disability prevention and management. We sought to derive and assess the predictive performance of rules to predict 3-year mortality and admission to acute care hospitals, SNFs, and LTC facilities among Medicare beneficiaries with differing ADL and IADL functioning levels.
Prospective cohort using Medicare Current Beneficiary Survey data from the 2001 to 2007 entry panels. In all, 23,407 community-dwelling Medicare beneficiaries were included. Multivariable logistic models created predicted probabilities for all-cause mortality and admission to acute care hospitals, SNFs, and LTC facilities, adjusting for sociodemographics, health conditions, impairments, behavior, and function.
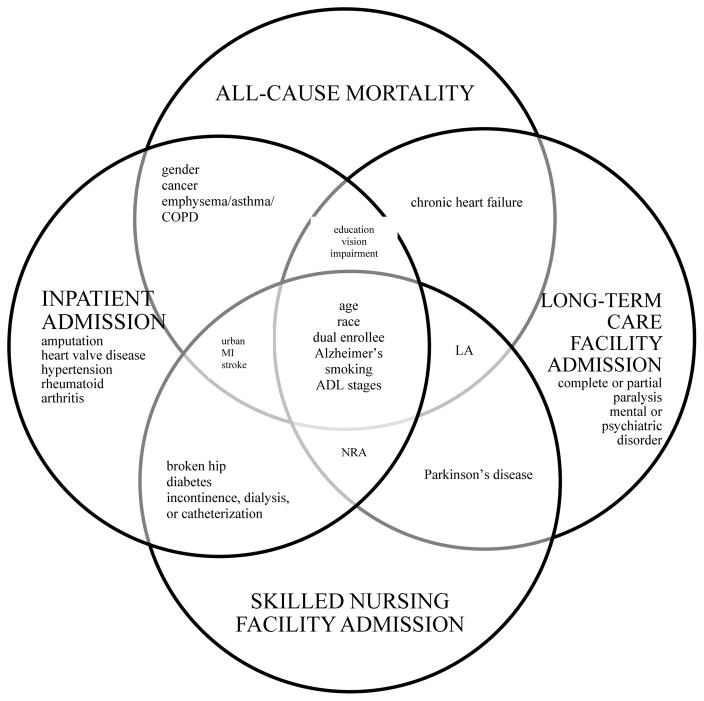
Sixteen, 22, 14, and 14 predictors remained in the final parsimonious model predicting 3-year all-cause mortality, inpatient admission, SNF admission, and LTC facility admission, respectively. The C-statistic for predicting 3-year all-cause mortality, inpatient admission, SNF admission, and LTC facility admission was 0.779, 0.672, 0.753, and 0.826 in the ADL activity limitation stage development cohorts, respectively, and 0.788, 0.669, 0.748, and 0.799 in the ADL activity limitation stage validation cohorts, respectively.
Parsimonious models can identify elderly Medicare beneficiaries at risk of poor outcomes and can aid policymakers, clinicians, and family members in improving care for older adults and supporting successful aging in the community.
预测老年人的死亡率和入住急性护理医院、熟练护理设施(SNF)和长期护理(LTC)设施的能力,以及其如何因日常生活活动(ADL)和工具性日常生活活动(IADL)状态而异,这可能有助于衡量旨在预防和管理残疾的经济、社会或卫生政策的成功或失败。我们试图推导和评估适用于不同 ADL 和 IADL 功能水平的 Medicare 受益人的规则,以预测 3 年死亡率和入住急性护理医院、SNF 和 LTC 设施的预测性能。
使用来自 2001 年至 2007 年入组小组的 Medicare 当前受益人体检数据进行前瞻性队列研究。共纳入 23407 名居住在社区的 Medicare 受益。使用多变量逻辑模型,根据社会人口统计学、健康状况、损伤、行为和功能,为所有原因死亡率和急性护理医院、SNF 和 LTC 设施入院创建预测概率。
在最终的简约模型中,有 16、22、14 和 14 个预测因子分别用于预测 3 年全因死亡率、住院入院、SNF 入院和 LTC 设施入院。ADL 活动受限阶段开发队列中,预测 3 年全因死亡率、住院入院、SNF 入院和 LTC 设施入院的 C 统计量分别为 0.779、0.672、0.753 和 0.826,ADL 活动受限阶段验证队列分别为 0.788、0.669、0.748 和 0.799。
简约模型可以识别处于不良结局风险中的老年 Medicare 受益人群,并有助于政策制定者、临床医生和家庭成员改善对老年人的护理,支持老年人在社区中的成功老龄化。