Rich Nicole C, Vartanian Shant M, Sharief Shimi, Freitas Daniel J, Tuot Delphine S
Department of Surgery, General Surgery Residency Program, U.C. San Francisco, 513 Parnassus Ave., S321, San Francisco, CA, 94143-0470, USA.
Department of Surgery, Division of Vascular & Endovascular Surgery, U.C. San Francisco, 400 Parnassus Ave., Suite A-501, San Francisco, CA, 94143, USA.
BMC Nephrol. 2017 Sep 2;18(1):279. doi: 10.1186/s12882-017-0700-9.
Despite improved health outcomes associated with arteriovenous fistulas, 80% of Americans initiate hemodialysis using a catheter, influenced by low socioeconomic status among other factors. Risk factors for incident catheter use in safety-net populations are unknown. Our objective was to identify factors associated with incident catheter use among hemodialysis patients at one safety-net hospital, with a goal of informing fistula placement initiatives targeted at safety-net populations more generally.
We performed a retrospective review of all incident hemodialysis patients at a single urban safety-net hospital from January 1, 2010 - December 31, 2015 (n = 241), as well as semi-structured interviews with a multi-lingual convenience sample of patients (n = 10) from this cohort. The primary outcome was incident vascular access modality. Multivariable logistic regression was used to identify factors associated with incident catheter use. Interview transcripts were coded using a directed content analysis framework based on a model describing barriers to healthcare access.
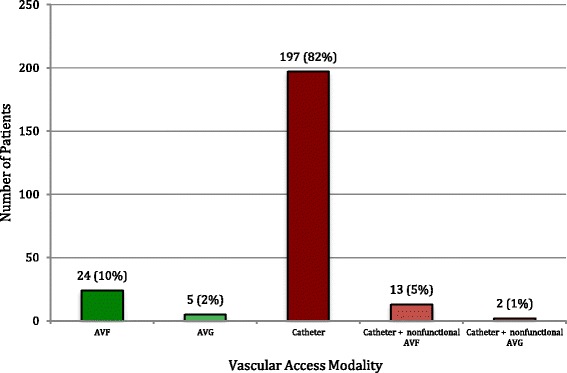
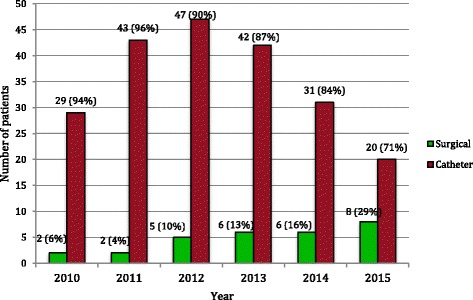
Subjects were 61.8% male, racially/ethnically diverse (19.5% white, 29.5% black, 28.6% Hispanic, 17.4% Asian), with a mean age of 52.4 years. Eighty-eight percent initiated hemodialysis using a catheter. In multivariable analysis, longer duration of nephrology care was associated with decreased catheter use (>12 months vs. 0-6 months: adjusted Odds Ratio [aOR] 0.07, 95% CI 0.02-0.23, p < 0.001), whereas uninsured status increased odds of catheter use (aOR 3.96, 1.23-12.76, p = 0.02). There was a decrease in catheter use after vascular surgery services became available in-hospital (OR 0.40, 95% CI 0.16-0.98, p = 0.04), however this association was not significant in multivariable analysis (aOR 0.48, 0.17-1.36, p = 0.17). During interviews, patients cited emotional responses to disease, lack of social and financial resources, and limited health knowledge as barriers to obtaining fistula surgery.
The rate of catheter use in this urban safety-net population is above the national average. Access to health insurance, early referrals to nephrology, and provision of in-hospital vascular surgery should be prioritized in the safety-net. Additionally, services that support patients' emotional and learning needs may decrease delays in fistula placement.
尽管动静脉内瘘可改善健康状况,但受社会经济地位低下等因素影响,80%的美国人开始进行血液透析时使用的是导管。安全网人群中初次使用导管的危险因素尚不清楚。我们的目标是确定一家安全网医院血液透析患者中与初次使用导管相关的因素,以便更广泛地为针对安全网人群的内瘘置入计划提供信息。
我们对一家城市安全网医院2010年1月1日至2015年12月31日期间所有初次进行血液透析的患者(n = 241)进行了回顾性研究,并对该队列中多语言便利样本的患者(n = 10)进行了半结构化访谈。主要结局是初次血管通路方式。采用多变量逻辑回归来确定与初次使用导管相关的因素。访谈记录使用基于描述医疗保健获取障碍模型的定向内容分析框架进行编码。
受试者中男性占61.8%,种族/族裔多样(19.5%为白人,29.5%为黑人,28.6%为西班牙裔,17.4%为亚洲人),平均年龄52.4岁。88%的患者开始血液透析时使用导管。在多变量分析中,肾病护理时间较长与导管使用减少相关(>12个月与0 - 6个月相比:调整后的优势比[aOR]为0.07,95%置信区间为0.02 - 0.23,p < 0.001),而未参保状态增加了导管使用的几率(aOR为3.96,1.23 - 12.76,p = 0.02)。医院提供血管外科服务后导管使用有所减少(优势比为0.40,95%置信区间为0.16 - 0.98,p = 0.04),然而在多变量分析中这种关联并不显著(aOR为0.48,0.17 - 1.36,p = 0.17)。在访谈中,患者提到对疾病的情绪反应、缺乏社会和经济资源以及健康知识有限是获得内瘘手术的障碍。
该城市安全网人群中导管使用率高于全国平均水平。安全网应优先考虑获得医疗保险、早期转诊至肾病科以及提供院内血管外科手术。此外,支持患者情绪和学习需求的服务可能会减少内瘘置入的延迟。